Feature | A Conversation with Anthony S. Fauci, MD, on COVID-19 and Influenza
By the time coronavirus cases started ticking up significantly in the U.S. in March and April, flu season had all but passed. This fall, the confluence of the two – COVID-19 and seasonal influenza – could push the health system to its limits.
Whatever the fall and winter brings virus wise, it will hit elderly patients who've likely seen their health status decline after months in lockdown and minimal medical care, an exhausted frontline workforce, and possibly patients made more vulnerable by existing or previous COVID-19 infection.
The ACC continues its commitment to informing patients with cardiovascular disease and their family and friends about one of the valuable steps they can take each year to optimize their health and prevent complications from vaccine-preventable diseases: get all their relevant vaccinations.
To gain some insight into what the cardiovascular community can do to help avert and best manage this potential tsunami, Cardiology spoke to the country's top infectious disease specialist, Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases.
Dr. Fauci, the 2018-2019 influenza season was considered a "moderate" one and still about 35.5 million Americans fell sick, 16.5 million went to a health care provider for their illness, and there were 490,600 hospitalizations and 34,200 flu-related deaths. That was with an influenza vaccination program that was functioning undisturbed and distributed almost 170 million doses. What's going to happen this year?

Fauci: That's a really interesting question because there are several potential scenarios that could play out. But I think we need to be honest and say upfront that we're really not sure what's going to happen. The worst-case scenario is we have a very active flu season that overlaps with the respiratory infection of COVID-19. Worst-case because that would really complicate matters from a diagnostic standpoint, from a therapeutic standpoint, and the standpoint of putting a lot of stress on the health care system.
There is also another possible scenario, which is something that epidemiologists who study respiratory infections occasionally see. In this other possible scenario, where there is an ongoing rampant respiratory illness, such as COVID-19, if another respiratory infection comes along such as seasonal influenza, there's only enough room in the niche of respiratory infections for one or the other. Thus, the rampant illness dominates, takes the niche and bumps out the other one.
We saw this in 2009 with the emergence of the novel pandemic H1N1 influenza virus. We started seeing widespread cases of H1N1 in the spring of 2009 and we were able to make a vaccine against it. But when the fall came, even though we had a vaccine for both H3N2 and H1N1, the H1N1 virus completely dominated the season and kicked the anticipated seasonal H3N2 off the map. Luckily, H1N1, although it was pervasive in transmission, it was kind of a wimpy virus and the deaths that year were even less than a regular seasonal flu year.
H1N1 and H3N2 are both influenza viruses, and one can argue that they are both competing for the niche of the sialic acid receptor on cells. However, there is another type of potential niche effect. If there is one type of virus that hits before another one (for example, SARS-CoV-2 vs. influenza), it could induce a degree of innate immunity that would be beneficial in fighting off the second virus. Again, my big caveat is that this is a speculation, not a prediction.
So, what are our options here?
Fauci: We need to use every tool we have. We have to get as many people vaccinated for influenza as we possibly can. At the same time, we need to make sure the clinical trials of the therapies we're developing for COVID-19 are done in an expeditious way, so we have the best possible interventions for COVID-19 as soon as possible.
It's been reported that the Southern Hemisphere is seeing about 90% fewer flu cases this year compared to last year, along with declines in other respiratory viruses, including respiratory syncytial virus and pneumococcal disease. What do you think are the reasons behind this decline and is it possible we'll see something similar here?
Fauci: I think it is possible that we're already seeing this epidemiological phenomenon that we just spoke of where the presence of COVID-19 itself might have a secondary effect of limiting the spread of other respiratory viruses. It's also very possible that better handwashing, masking and physical distancing is slowing the spread of these other viral illnesses. And it could be both of these going on at the same time.
Might this dynamic of falling flu incidence, whatever the reasons, make it less crucial to vaccinate so many people against influenza?
Fauci: Absolutely not. We still need to vaccinate as many people as possible. You don't want to get COVID-19 and you don't want to get influenza either.
Any worries that the vaccine supply chain might be disrupted this year?
Fauci: No, we're going to deliver the seasonal influenza vaccine the same way we do every year. The vaccines will be commercially available and given at the doctor's office, in pharmacies, and all the different places it's usually given.
Given that some of the usual ways in which we make sure to vaccinate large numbers of citizens against seasonal influenza may be diminished, do you foresee or are there plans being made for non-traditional ways of getting high vaccination rates (e.g,. drive-thru flu shots)?
Fauci: Not really. What we're hoping for, and I'm cautiously optimistic about this, is that by adhering to the public health measures we've suggested for COVID-19, we will not be as shut down as we have been and as we open up the country, people will go back to having normal access to their physicians. Of course, some of these places – the doctor's offices and pharmacies – may adjust their practices to make it safer for people to come and get vaccinated.
The U.S. Centers for Disease Control and Prevention (CDC), as well as several other countries, have taken a transmission-based, universal vaccination approach to limit disease burden, recommending yearly influenza vaccination for everyone six months and older. This is based on the idea of herd immunity and evidence that vaccine effectiveness may be lower in some higher-risk groups, like individuals with heart failure and the elderly. Are you advocating for the same flu vaccine strategy as in the past or are you modifying it, and if so how?

Fauci: The guidance remains the same. Everyone six months of age and older should get vaccinated, with a particular emphasis on the higher-risk groups, small children, pregnant women, the elderly, and those with underlying conditions.
Once flu season starts, how will we even know which illness we're dealing with? Will the labs and hospitals have the capacity to test for both flu and COVID-19? Or will we be working under assumptions based on prevalence of COVID-19?
Fauci: I hope by the time we get to the fall the problems we've seen with testing availability and turnaround time will be solved and people will be able to go to a doctor's office and get tested for both influenza and COVID. It's not standard right now, but there are a number of companies that have started to work on a test that can test for both of them simultaneously.
Is this a unique diagnostic challenge or is this not uncommon in the world of infectious diseases?

Fauci: I would say that this is unprecedented. There are other respiratory infections that can co-circulate and be tricky to diagnose during flu season, but the outbreaks are minor and not of epidemic proportions, like influenza. We haven't had a situation with this kind of potential, where we might have two illnesses, one that is of epidemic proportions and the other pandemic, co-circulating at the same time. It's going to be a unique experience, and, as I mentioned before, we're really not sure how it will actually play out.
What message(s) should cardiovascular professionals be sending to their patients to help prepare them for the fall and winter season and a possible second wave? Is it a different message for different populations?
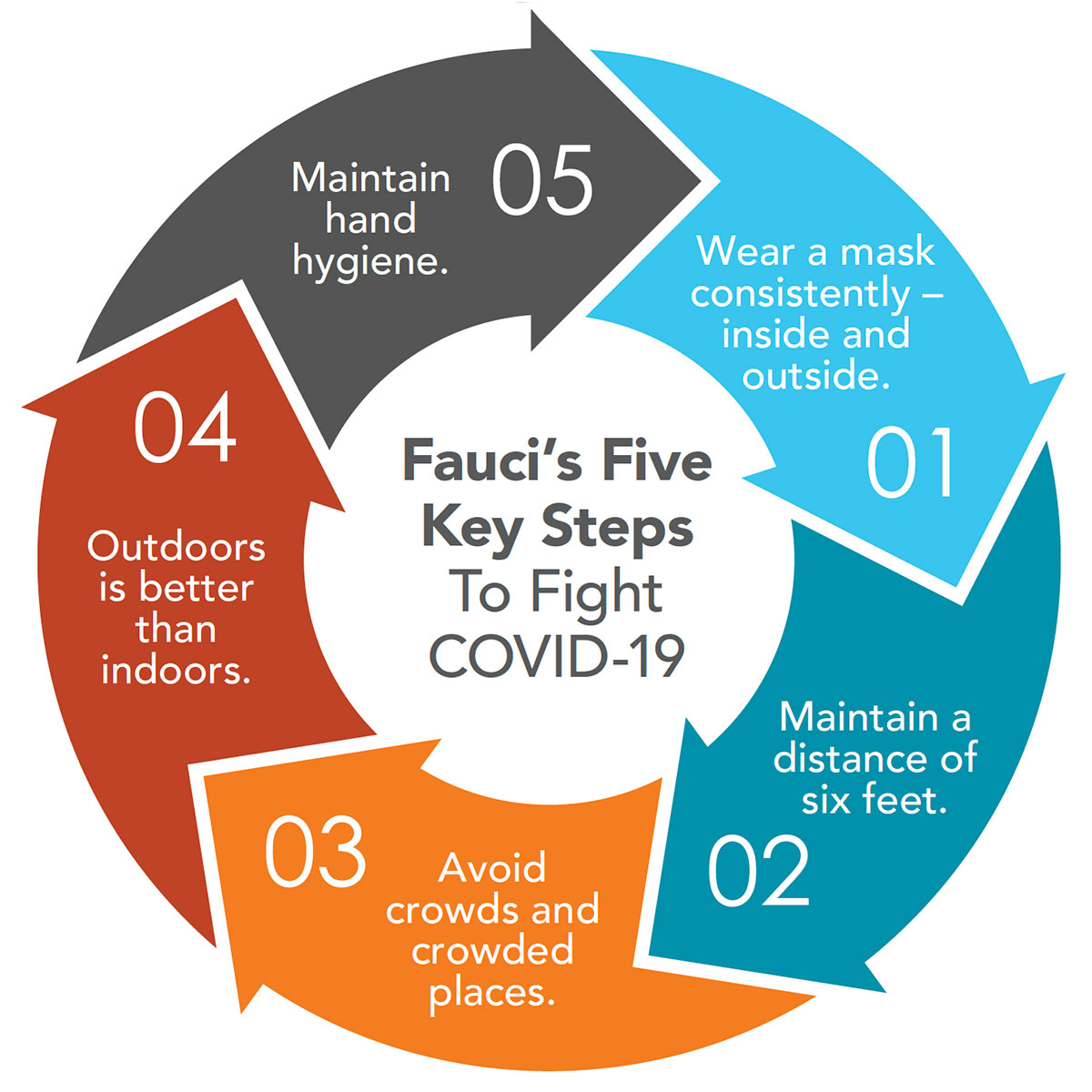
Fauci: We need to make sure we get across that the things we should be doing for the containment of COVID-19 are directly applicable to influenza as well. Wearing a mask consistently indoors and outdoors, keeping a distance of six feet, avoiding crowds, and avoid crowded places like bars – and in fact, maybe even close the bars in some places. Outdoors is always better than indoors, recognizing that will be more difficult as the weather gets colder. And hand hygiene is critical too. I keep repeating these five steps because it's what we really need to all be doing and what we should be stressing to patients, especially those who are more vulnerable.
Cardiovascular disease patients – where do you think they'd fall on the priority list for vaccination once a COVID-19 vaccine is available?
Fauci: Likely quite high. The ultimate decision on prioritization will be made in the standard way we do it each year, which is that ACIP – the Advisory Committee on Immunization Practices – which reports directly to the CDC, will make their recommendations for prioritization. The CDC generally takes their recommendations, but in this case, understanding this will be controversial and it will not be possible to immediately vaccinate everyone right away, there will be an added layer of deliberation, in that a committee with representatives of the National Academies of Sciences, Engineering, and Medicine and the National Academy of Medicine will also provide their expert opinion. This committee was requested by the NIH and the CDC to compliment the deliberations of the ACIP regarding prioritization of any COVID-19 vaccine that is developed.
Older folks have received consistent messages about the importance of receiving vaccination against influenza, pneumonia and shingles, among other things. As we think about vaccination for COVID-19, will there be an approach taken to ensure older Americans receive all the vaccines they need, both from an infrastructure approach and in terms of messaging?
Fauci: Given that older adults are at increased risk for severe illness if they get COVID-19, that will likely factor in to decisions regarding vaccine prioritization and distribution. It is critical that we continue to message the importance of receiving vaccinations to vulnerable populations, including older adults.
Changing gears a little bit, we've seen that COVID-19 is a maddeningly multi-organ condition. One year from now, which medical subspecialty do you think will be most involved in the management of long-term sequelae of COVID-19?
Fauci: Oh, that's an excellent question. We are seeing more and more people who have cleared their infection, but who then have longer-term consequences and chronic, somewhat debilitating conditions. We're going to have to take these issues seriously and work to understand better what's happening.
I'm not sure of the specific answer to your question, but we're very clearly seeing that there are concerning cardiovascular complications related to infection with SARS-CoV-2. There are cases we've seen where young, completely healthy people have developed cardiomyopathies and died. And now on autopsy, we're seeing virus in some of the small vessels in the heart. So, I think the heart is a real target for this virus that has not been completely appreciated.
Did you see the article in JAMA Cardiology last week that looked at signs of myocardial involvement and inflammation on cardiac magnetic resonance imaging in COVID-19 survivors, most of whom were relatively young and recovered out of hospital?
Fauci: I did and it was very sobering. Understanding the longer term sequelae of this virus is critically important.
Given what you've seen in this current, unprecedented crisis, has your general approach to infectious diseases in general changed?
Fauci: Not really because, unfortunately, this is something I've been lecturing on for decades – the dangers of emerging infectious diseases and how my worst nightmare scenario would be to have the emergence of a respiratory infection that jumped species from an animal host to a human, and with two fundamental characteristics met: very efficient transmission from human to human and a high degree of morbidity and mortality in at least a subset of people. In this case, that subset is the elderly and those who have underlying conditions, including cardiovascular disease. So, I'd like to say this was a surprise, but it wasn't entirely.
Any predictions on how the Nationals will fare this season? There's a lot of fans at the ACC!
Fauci: The Nats will again be World Series champions!

Clinical Topics: Acute Coronary Syndromes, Anticoagulation Management, Arrhythmias and Clinical EP, Cardiac Surgery, Cardiovascular Care Team, Congenital Heart Disease and Pediatric Cardiology, COVID-19 Hub, Diabetes and Cardiometabolic Disease, Dyslipidemia, Geriatric Cardiology, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Pericardial Disease, Prevention, Pulmonary Hypertension and Venous Thromboembolism, Sports and Exercise Cardiology, Stable Ischemic Heart Disease, Valvular Heart Disease, Vascular Medicine, Anticoagulation Management and ACS, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Cardiac Surgery and Arrhythmias, Cardiac Surgery and CHD and Pediatrics, Cardiac Surgery and Heart Failure, Cardiac Surgery and SIHD, Cardiac Surgery and VHD, Congenital Heart Disease, CHD and Pediatrics and Arrhythmias, CHD and Pediatrics and Imaging, CHD and Pediatrics and Interventions, CHD and Pediatrics and Prevention, Acute Heart Failure, Pulmonary Hypertension, Interventions and ACS, Interventions and Imaging, Interventions and Structural Heart Disease, Interventions and Vascular Medicine, Angiography, Nuclear Imaging, Hypertension, Sleep Apnea, Sports and Exercise and Congenital Heart Disease and Pediatric Cardiology, Sports and Exercise and ECG and Stress Testing, Sports and Exercise and Imaging, Chronic Angina
Keywords: ACC Publications, Cardiology Magazine, COVID-19, severe acute respiratory syndrome coronavirus 2, Coronavirus, Pandemics, Influenza A Virus, H1N1 Subtype, Aged, Influenza Vaccines, Influenza, Human, Influenza A Virus, H3N2 Subtype, Immunity, Herd, Respiratory Syncytial Viruses, Incidence, Public Health, Hand Disinfection, Pharmacies, Pharmacies, Pregnancy, Communicable Diseases, Emerging, Prevalence, Advisory Committees, Vulnerable Populations, Cardiovascular Diseases, Hand Hygiene, Expert Testimony, Autopsy, National Academy of Sciences, U.S., Acute Coronary Syndrome, Anticoagulants, Arrhythmias, Cardiac, Cardiac Surgical Procedures, Metabolic Syndrome, Angina, Stable, Heart Defects, Congenital, Dyslipidemias, Geriatrics, Heart Failure, Angiography, Diagnostic Imaging, Pericarditis, Secondary Prevention, Hypertension, Pulmonary, Sleep Apnea Syndromes, Sports, Angina, Stable, Exercise Test, Heart Valve Diseases, Aneurysm
< Back to Listings