Cover Story | Cardiology and the Drug Abuse Crisis: Points of Intersection

It may feel like old news already, but the drug abuse crisis in the U.S. is far from over. In fact, it hasn't even peaked yet, despite the fact that most of the worst excesses of marketing and liberal prescribing have stopped.
Most of those working in cardiology have been sheltered from the worst of this public health emergency, but there are some specific areas of impact and these are reviewed here.
In 2017, there were 71,237 overdose deaths in the U.S., 47,600 (67.8 percent) of those involving opioids.1 This is up from 2016, which was up from 2015.
And it's not just natural opioids. Drug overdose deaths have increased also with synthetic opioids (other than methadone), cocaine, methamphetamines, heroin and other narcotic drugs. Indeed, while opioids have gotten most of the attention, nonopioid overdose death rates have risen almost as fast as those involving opioids.
The actual numbers, as recently reported in Health Affairs, are alarming: between 1999 and 2016, a 274 percent increase in nonopioid drug deaths and a 371 percent increase in opioid drug deaths.2
"We haven't seen the peak yet. I think we're cresting, we're getting to the point where we are maybe going to start making some progress towards getting to the peak, but it's still going to get worse before it gets better," says Craig J. Beavers, PharmD, an associate member of the ACC and co-chair of ACC's clinical pharmacist workgroup.
Infective Endocarditis

Infective endocarditis (IE) has traditionally been considered a rare disease, but in those places hit hardest by the drug abuse epidemic, hospitals are seeing many more cases of injection drug use (IDU) IE.
Intravenous (IV) drug abuse and infectious disease are inextricably linked:
- Viral infections are transmitted through high-risk injection practices
- Transmission of human immunodeficiency virus (HIV) and hepatitis C virus (HCV) also occur through drug-related high-risk sexual risk behavior; and
- If that's not enough – the drugs themselves are often contaminated with bacterial and fungal pathogens, which can spread throughout the body and cause infections such as IE.3
There's even emerging evidence that some opioid drugs have putative effects on innate and adaptive immunity.3
The true incidence of IE, either before or after this current wave of drug-related IE, is hard to pin down. But there is evidence that trends in IDU-IE hospitalizations appear to track closely with the prescription opioid, heroin, HCV and overdose epidemics seen regionally.4,5
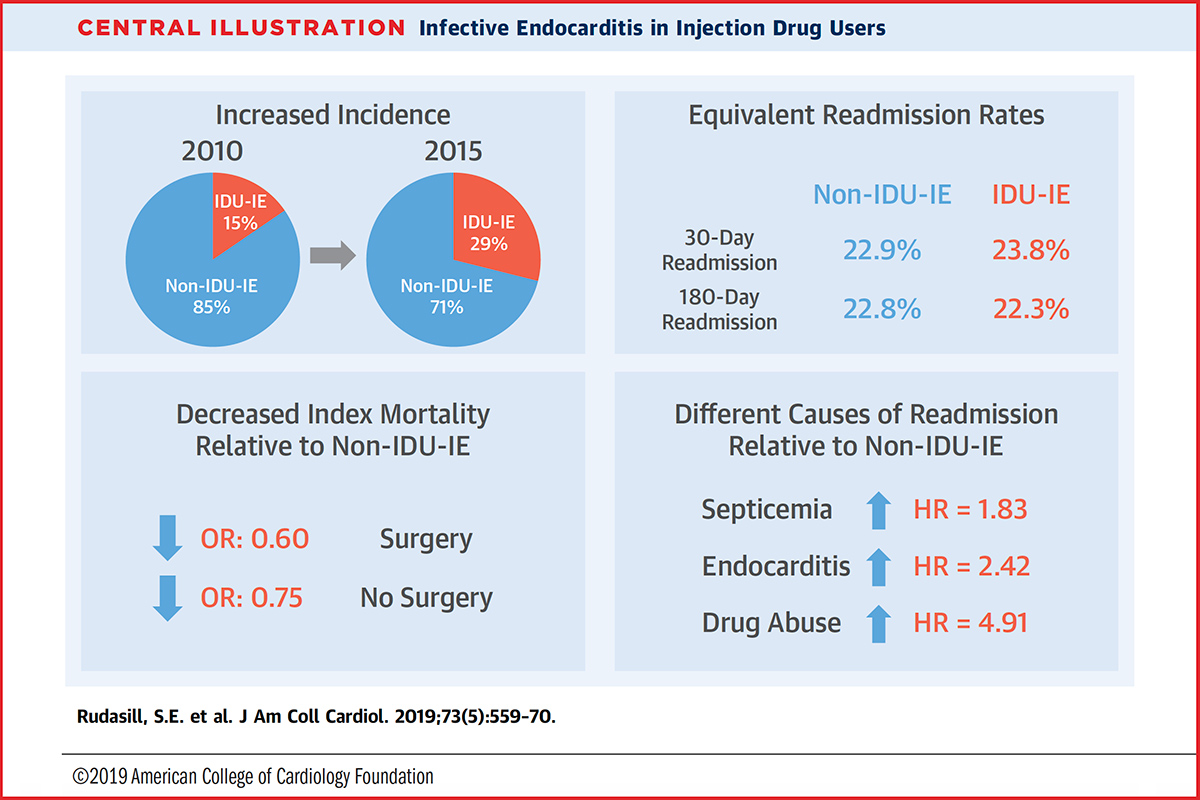
A recent study in the Journal of the American College of Cardiology took a close look at trends associated with IE associated with IDU.6 In a survey-weighted sample from the National Readmissions Database (NRD), there were 27,432 cases of IDU-IE between January 2010 and September 2015, and 96,344 cases of non–IDU-IE. During this period, the proportion of all IE cases ascribed to IDU rose from 15.2 percent to 29.1 percent.
As expected, those with IDU-IE were younger and had fewer comorbidities compared with non–IDU-IE. Those in the 15- to 34-year age group were at the highest risk, with 46.7 percent of all IDU-IE cases in this age group by 2015.
Individuals with IDU-IE had reduced mortality compared with those with non–IDU-IE (6.8 percent vs. 9.6 percent; p<0.001), likely reflective of them being younger and generally healthier, but similar 30-day readmission (23.9 percent vs. 22.9 percent; p=0.077).
About 11 percent of both groups underwent valve surgery, most often to replace the mitral or aortic valves. In most cases (81 percent) only one valve was treated.
"I think the decision to operate the first time is usually fairly straightforward. But it's the re-do valve operations, when the prosthetic valve gets infected because of continued drug use, where people are struggling. I believe there are some surgeons who say they won't re-operate on these patients and others who do," says Mary Norine Walsh, MD, MACC, medical director, heart failure and cardiac transplantation at St. Vincent Hospital in Indianapolis, IN, and past president of ACC.
 Click the image above for a larger view.
Click the image above for a larger view.
When managed medically, those with drug-related IE had significantly longer hospital stays and were more likely to be readmitted for endocarditis (18.1 vs. 5.6 percent), septicemia (14.0 vs. 7.3 percent) and drug abuse (4.3 vs. 0.7 percent), as compared with those with non–IDU-IE (Figure 1).
When managed surgically, they also required greater resource use with longer length of stay, and more readmissions for septicemia and drug abuse.
Beavers explains some of the struggles hospitals are having treating these patients. "It's very resources intensive. Besides possibly needing valve surgery, these patients need four- to six-weeks of IV antibiotics, and we really can't send them home with a central line for the antibiotics because we're literally giving them easy access to their bloodstream," says Beavers.
Walsh believes this way of thinking may actually be counterproductive. "I think it's very paternalistic. You don't need a picc line to shoot up drugs. And just because you have an individual in whom you have now invested a certain amount for a valve replacement, aren't you hoping for redemption and believing they'll stop using?"
"On the contrary, I believe keeping them in the hospital for something that's outpatient therapy reinforces the belief that they will go back to the drugs. This is a personal opinion and I don't know if it's shared by others," she says.
Licit Use of Opioids in Cardiology
There was a time when opioids had some indications in cardiology, but those days have passed, according to Walsh.
"The only cardiologists who might still send a patient out of the hospital with a prescription for opioids are electrophysiologists, because they'll do a skin incision to put a pacemaker or defibrillator in," she says. "I used to routinely refill prescriptions for patients who had previous cardiac surgery, but these days I send them either back to the prescribing surgeon or to their primary care doctor."
"I think the difference now is that we are looking more at the evidence for other nonopioid modalities of pain control, and thinking about getting people into rehabilitation and physical therapy quicker because those things help alleviate pain," says Beavers.
He adds that for most indications in cardiology, opiates are not recommended or effective.
Even in STEMI, opiates are still in the guidelines for analgesia, "but I don't think people are using them much even in the acute setting, because we want to be good stewards of opioid use, but also because we know opiates slow absorption of some medications, like the P2Y12 inhibitors, and may inhibit antiplatelet activity. There is also concern that they may mask the pain of a worsening infarction, delaying treatment."
"It's really about protecting our patients, but also their families because we know now that just having a family member on a prescription opioid increases the risk for household family members," says Walsh.
The Silver Lining: Hearts For Transplant

Aside from the marked increases in IE, perhaps the greatest intersection with cardiology and the drug-abuse crisis is the greater availability of hearts for transplantation. Not only are more overdose-related hearts being recovered, but transplant specialists are more comfortable using them for transplant as they gain more experience and see that the organs are safe.
Recently, Mandeep Mehra, MD, Msc, FACC, at Brigham & Women's Hospital, and colleagues published data showing an increase in heart transplantation in the U.S. over the past 15 years, driven by about an 11-fold increase in the proportion of organ donors who died from drug intoxication.7
A look at the Organ Procurement and Transplantation Network (OPTN) data is telling: in 2000, the percentage of adult donors who died from drug intoxication from whom hearts were recovered for transplantation was 1.1 percent (25 of 2,284 donation hearts). In 2018, that number had risen to 18.3 percent (633 of 3,466 donor hearts).
Mehra and colleagues used OPTN data to further determine net annual changes in the size of the heart transplant wait list (the number of new registrations minus the total number of removals).8 While causality cannot be determined, it appears this rise in organs recovered from lives lost to drug intoxication may be tied to a decrease in the size of the waiting list for heart transplantation.
Regarding the long-term viability of these hearts, the data so far looks positive. About one-fifth of organ donors who died from an overdose are HCV positive (HCV+). Traditionally, these organs would not be considered for transplantation, but direct acting antiviral (DAA) drugs, which are curative of HCV infection, have heralded a new era in organ donation from HCV+ donors.
The largest single-center experience to date of HCV+ transplantation comes from Vanderbilt University Medical Center in Nashville, TN. Kelly Schlendorf, MD, presented their findings at the International Society for Heart and Lung Transplantation meeting in April.9
In 74 patients who received an HCV+ heart between August 2016 and March 2019, 63 were nucleic acid amplification test (NAT) positive (viremic load was detected). Sixty of these became viremic and 41 have completed DAA treatment with 100 percent viral clearance and sustained virologic response at 12 weeks from treatment cessation.
Of note, median wait time for a heart was only four days, reported Schlendorf. One-year survival was 83 percent, compared with 90 percent for those who received non-HCV hearts (p=NS). They've seen no issues with graft dysfunction or rejection, stroke or liver failure, but two patients developed necrotizing pancreatitis during the viremic phase which responded to DAA treatment.
"The ability to treat hepatitis C has clearly expanded the donor population, but what we really need to see is coverage of the antiviral drugs by insurance companies," says Walsh. "Some centers treat prophylactically. At St. Vincent, we wait until there is a serologic diagnosis. We find this works well, but even in that case, where we have a patient who has undergone heart transplantation and is now HCV+, the insurance companies don't want to pay for the DAAs."
"We have spent hours and hours in discussions with insurers to get these drugs paid for in order for our team to continue to do these transplants," she adds. Some centers are using grant money to pay for the drugs.
The days of plentiful donor hearts from drug-related deaths may be coming to an end, according to Beavers. Greater availability of the opioid reversal agent naloxone in the community is slowly having an effect of death rates.
"I've seen changes across the states, greater comfort with the reversal agent, and protocols developed where pharmacists in local retail pharmacies have access to naloxone and can give it when needed," says Beavers.
Hence his feeling that this crisis is close to peaking and may see the other side of the curve before too much longer.
Tracing the Origins of the Opioid Crisis

Why did the opioid crisis affect the U.S. more than other countries? The simple answers are shady marketing, "pill mills" and liberal prescribing by U.S. physicians. But in a recent talk, Mandeep Mehra, MD, MSc, FACC, from Harvard Medical School and editor-in-chief of the Journal of Heart and Lung Transplantation, took the discussion a few steps further. He asked what other factors provided such fertile ground for injudicious prescribing of these drugs. He gives three primary reasons.
The first: in 1980, a letter to the editor was published in the New England Journal of Medicine by Porter and Jick from the Boston Collaborative Drug Surveillance Program at Boston University Medical Center. In this now infamous letter – which was exactly five sentences long – the authors discussed their chart review looking at the incidence of addiction among 18,882 hospitalized medical patients prescribed a narcotic.10
Here's their final sentence: "We conclude that despite widespread use of narcotic drugs in hospitals, the development of addiction is rare in medical patients with no history of addiction."
"According to a bibliometric analysis from 2017,11 this letter was cited more than 600 times between 2000 and 2017, and about 72 percent of those citations were affirmational, meaning it was used as evidence that addiction risk is low with opioids," says Mehra in an interview. "Most of the citations, about 80 percent, didn't specify that the patients studied were inpatients when they received the prescription, rather it was misrepresented and used for very focused marketing by drug companies."
Another reason this uniquely American crisis progressed as it did, says Mehra, had to do with a "scathing report" released in 2000 by the Joint Commission of the Accreditation of Healthcare (JCAHO), which said that doctors weren't controlling pain adequately in all hospitals and nursing homes. Following this report, JCAHO (now called The Joint Commission) set standards that required greater monitoring and treatment of pain.
These new standards were applicable to all organizations accredited by JCAHO – ambulatory care, behavioral health, health care networks, home care, hospitals, long-term care and long-term care pharmacies – and were consistent with the positions of The American Pain Society and the U.S. Veteran Health Administration's "Pain: The Fifth Vital Sign."12
"Every time they accredited a hospital system in the U.S., they actually looked to see how good the pain control was and so, of course, doctors started prescribing more and more opioids," says Mehra.
"I don't think other countries officially made pain a performance measure, nor do they have the same type of accreditation standards that we have in the U.S., where a hospital lives or dies by its Joint Commission accreditation," he adds.
Total opioid prescriptions were rising before the new standards were released, and continued to rise. From 2000 to 2013, the annual number of prescription opioids dispensed by U.S. retail pharmacies rose from 126 million to 219 million.13
Added to all this, is an economic phenomenon that has been dubbed "deaths of despair," developed by economists Sir Angus Deaton and Anne Case, both from Princeton University.
In a 2015 paper in PNAS, Deaton, a Nobel Prize winner, and Case tracked the increased numbers of middle-aged, white Americans dying largely from drug and alcohol poisonings, suicide, and chronic liver disease and cirrhosis in recent years.14 Born of low educational achievement and income inequality, this segment of the population has seen a reversal in decades of progress in mortality. Their increase in all-cause mortality in midlife has not been seen in any other rich country.
Indeed, even in the U.S., only the white, non-Hispanic segment of the population saw a reversal in midlife mortality; black non-Hispanics and Hispanics at midlife, and those aged 65 and above in every racial and ethnic group continue to see falling mortality, Deaton and Case show.
"The bottom line is that we have a problem with the fact that socioeconomic conditions and depression, lack of employment, et cetera, have become social variables that determine easy conversion into addiction," says Mehra. "These were all well-minded things that people said or did that actually were weaponized, either directly or indirectly and subsequently resulted in a poor outcome. It's a sad story, but a fascinating one too," he adds.
References
- Scholl L, Seth P, Kariisa M, et al. MMWR Morb Mortal Wkly Rep 2019;67:1419-27.
- Ruhm CJ. Health Affairs 2019; 38:1216-24.
- Schwetz TA, Calder R, Rosenthal E, et al. J Infect Dis 2019;April 3:[Epub ahead of print].
- Keeshin SW, Feinberg J. Am J Med Sci 2016;352:609-14.
- Wurcel AG, Anderson JE, Chui KK, et al. Open Forum Infec Dis 2016;3:ofw157.
- Rudasill SE, Sanaiha Y, Mardock AL, et al. J Am Coll Cardiol 2019;73:559-70.
- Mehra MR, Jarcho JA, Cherikh W, et al. N Engl J Med 2018;378:1943-5.
- Vaduganathan M, Machado SR, DeFillipis EM, et al. N Engl J Med 2019;380: 597-9.
- Schlendorg K, Zalawadiya S, Shah A, et al. Abstract #96. Presented at ISHLT 2019; April 2019.
- Porter J, Jick H. N Engl J Med 1980;302:123.
- Leung PTM, Macdonald EM, Stanbrook MB, et al. N Engl J Med 2017;376:2194-5.
- Department of Veterans Affairs. Pain: The Fifth Vital Sign. October 2000. Available here. Accessed June 27, 2019.
- Baker DW. The Joint Commission's Pain Standards: Origins and Evolution. Available here. Accessed on June 27, 2019.
- Case A, Deaton A. Proc Natl Acad Sci USA 2015;112:15078-83.
Clinical Topics: Arrhythmias and Clinical EP, Cardiac Surgery, Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Implantable Devices, SCD/Ventricular Arrhythmias, Aortic Surgery, Cardiac Surgery and Arrhythmias, Cardiac Surgery and Heart Failure, Acute Heart Failure, Heart Transplant
Keywords: ACC Publications, Cardiology Magazine, Academic Medical Centers, Adaptive Immunity, Analgesia, Anti-Bacterial Agents, Analgesics, Opioid, Antiviral Agents, Aortic Valve, Cocaine, Communicable Diseases, Comorbidity, Defibrillators, Drug Overdose, Endocarditis, Heart Failure, Heart Transplantation, Hepatitis C, Hepacivirus, Heroin, HIV Infections, Infarction, Liver Failure, Methamphetamine, Methadone, Lung Transplantation, Naloxone, Nucleic Acid Amplification Techniques, Opiate Alkaloids, Outpatients, Pacemaker, Artificial, Pain, Pancreatitis, Patient Readmission, Pharmacies, Pharmacists, Physician Executives, Primary Health Care, Public Health, Rare Diseases, Myocardial Infarction, Stroke, Risk-Taking, Substance Abuse, Intravenous, Substance-Related Disorders, Tissue and Organ Procurement, Tissue Donors, Withholding Treatment
< Back to Listings