Feature | ACC's Governance Transformation: Poised to Meet Our Mission
 William A. Zoghbi, MD, MACC
William A. Zoghbi, MD, MACC
 W. Douglas Weaver, MD, MACC
W. Douglas Weaver, MD, MACC
 Athena Poppas, MD, FACC
Athena Poppas, MD, FACC
The ACC has continuously evolved and dramatically expanded over the last 70 years; growing in size and scope to meet the changing needs of the entire cardiovascular workforce and ultimately improve the lives of patients living with or at risk of heart disease around the world.
Given all this change, the ACC has worked over the last several years to transform its governance structure and processes to best position the College to achieve its Mission of transforming cardiovascular care and improving heart health.
The governance transformation was a slow and deliberate process that grew out of a series of meetings, conversations and a critical look at the health care environment in 2014 led by William A. Zoghbi, MD, MACC, and W. Douglas Weaver, MD, MACC.
The establishment of an official Governance Committee chaired by Athena Poppas, MD, FACC, followed in 2016, with the goal of phasing in structural and process changes designed to make the ACC more nimble, strategic, accountable, competency-based, and reflective of the diversity and breadth of the cardiovascular community.
The Road to Transformation
ACC's governance transformation was anchored by a set of 11 Governance Principles (see sidebar). The Principles – BOT best practices – supported the overarching desire for a smaller Board of Trustees (BOT) with centralized authority, but decentralized decision-making via member groups like committees, sections, etc.
ACC's Governance Principles
I. Governance Function
- The Board is strategically oriented to support the Mission.
- Governance focus is on strategy and policy, and not on tactical, implementation or management issues.
- Governance shall operate on the principle of: centralized authority and decentralized decision-making.
- The Board must ensure it is aware of the needs and challenges of all the members of the College as it relates to the Mission, and has multiple mechanisms and avenues for membership voice to be heard at the Board level.
II. Governance Structure
- Governance structure supports optimum governance function and efficiency, and so Board size and other structural components shall be consistent with best practice evidence and thinking.
- The Board is the ultimate authority of the College. It appoints an Executive Committee which reports to and is controlled by the Board and has a new explicit charter of its role and authority.
- The Board determines and maintains appropriate committees with clearly defined roles, functions, authority and accountability, and appoints the members of these committees.
- A majority of the members of the Board shall be members of the College.
- The Board shall seek diversity in its membership including but not limited to: expertise; experience; gender; race; geographic location; and age.
- There shall be a competency-based selection model for composition of the Board, and the committees of the Board.
- Board members shall not concurrently serve as chairs or members of nonstanding (major operating) committees of the College. (For a list of the nine nonstanding committees, see Number Check.)
Key tactics included phasing in a smaller board over a three-year period, developing core leadership competencies (Figure 1) to guide the application and selection process of ACC leaders; and updating and clearly defining leadership position descriptions.
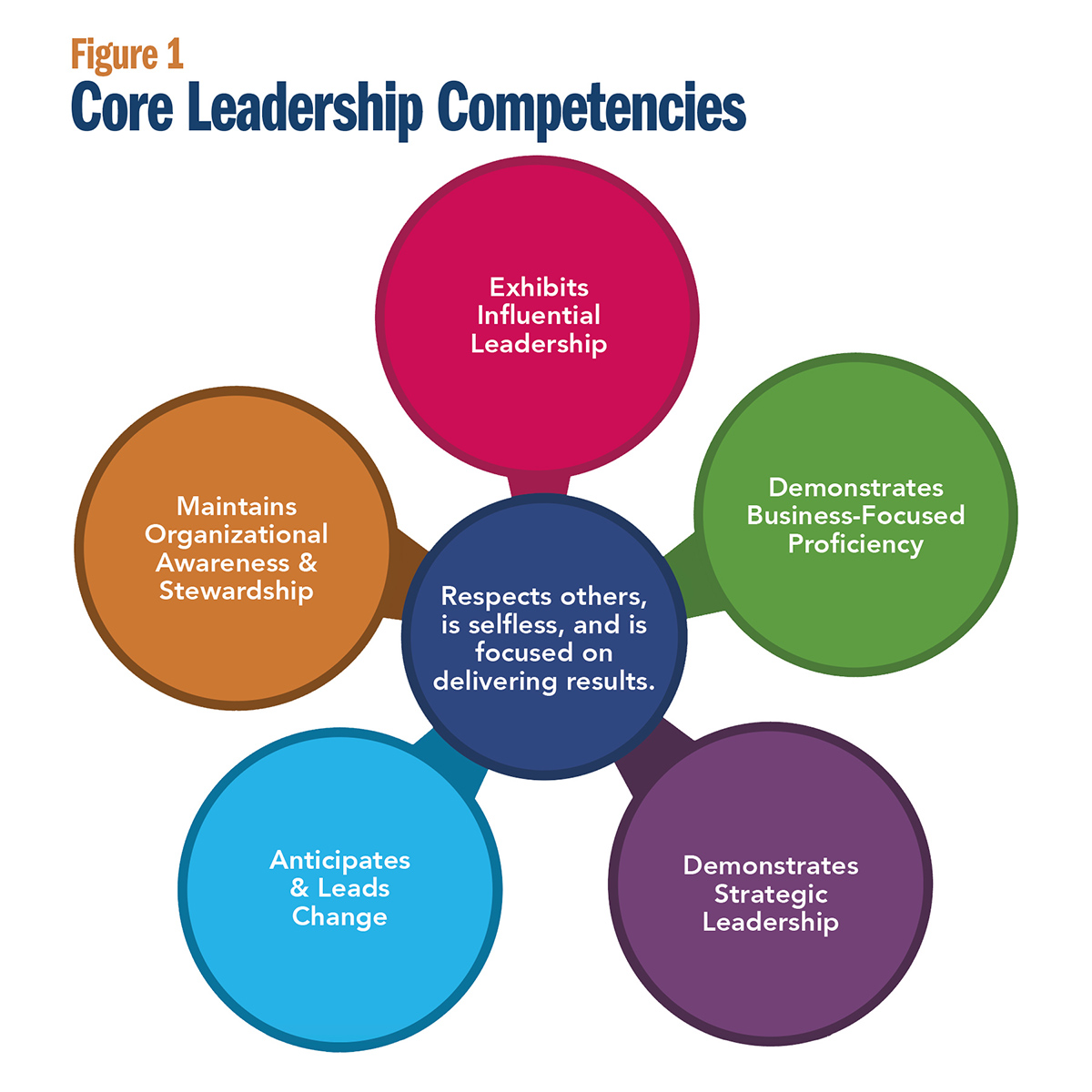 Click the image above for a larger view.
Click the image above for a larger view.
Additionally, an "Authority Matrix" to illustrate the meaning and process of centralized authority and decentralized decision-making needed to be created and refined; committee and council charters needed to be reviewed; and robust member leadership development needed to be put in place.
Implementing these Principles wasn't a simple process. It required much learning, listening and inevitable course-correcting to ensure the College was on the right track. According to Poppas, some of the greatest challenges along the way were to be expected – especially given that the governance process and structure had not changed for two decades.
 Huon H. Gray, MD, MACC
Huon H. Gray, MD, MACC
 Joseph G. Cacchione, MD, FACC
Joseph G. Cacchione, MD, FACC
 Michael J. Mack, MD, FACC
Michael J. Mack, MD, FACC
"The first challenge was acceptance among leaders," she said. "Operationalizing a smaller board, building and disseminating our core competencies, and creating understanding and functioning of decentralized decision-making were hurdles – the latter of which require ongoing work."
In some cases, particularly in transitioning to a much smaller board, several College leaders volunteered to end their terms on the Board of Trustees early.
"Voting for one's own redundancy is never easy, especially when service on the Board is so highly prized and such a privilege," says Huon H. Gray, MD, MACC, who currently serves as the chair of ACC's Governance Committee.
"But in truth, it was obvious that the Board was too large for all members to feel fully engaged and be contributory. Too often we would become immersed in tactics rather than strategy. The Governance Task Force's recommendations for change came as no surprise. Those of us who served shorter terms as a consequence were simply helping ensure a speedy transition to a better system of governance."
Since then, the BOT has transitioned from 31 members to its current 14 members, including ACC's Immediate Past President, the Board of Governors Chair-Elect and a new Membership Committee Chair. According to ACC Trustee Michael J. Mack, MD, FACC, reducing the number of Board members and increasing the frequency of Board meetings have contributed to greater engagement and effectiveness of the Board.
— Joseph G. Cacchione, MD, FACC
Past Governance Committee Member and Trustee Joseph G. Cacchione, MD, FACC, agrees. "ACC's governance transformation has enabled the organization to be more efficient and nimble than ever before. The model of a Board focused on governance and strategy, as opposed to tactics and management, empowers ACC to align with governance best practices and, more importantly, will make us a more effective organization as we work to meet our Mission of transforming cardiovascular care and improving heart health."
Shaping the Future
The governance transformation was a long process, but the College is now poised to best ensure its serving today's members. "Change is difficult for individuals and organizations," says Poppas, "but by explaining the "why" and the "how," building trust and working together, the process moved forward."
Poppas and others note there are now more positions available to a wider group of members, allowing for greater independence, diversity and vibrancy of committees and councils. Where in 2016 there were 188 leadership positions to fill, this number has grown to 325 today.
Additionally, as part of the transformation process, Board Members cannot concurrently serve as chairs or members of nonstanding committees of the College, says Poppas, allowing for increased leadership opportunities for others.
Continuing to build a pipeline of leaders at the College and in cardiovascular medicine is a priority of the governance transformation – in line with ACC's Strategic Plan.
"There is a strong commitment to ensure as much opportunity as possible for those members who wish to serve in the volunteer roles available, and that best practice is followed with regard to diversity and inclusion," says Gray.
The College has been working to establish systems by which members from all backgrounds and career stages can see where opportunities exist and that application processes are clear. Already, work has been done to upgrade the application process to allow members to apply to multiple committees and positions within one system.
"It is our collective responsibility to encourage members to participate in College activities, and to support and develop them in their new roles. If we do this, the College will achieve its ambition to be the professional home of the entire cardiovascular team," Gray says.
— Huon H. Gray, MD, MACC
Looking ahead, the College is working to establish clearer and more robust lines of communication and clarify what the new Governance structure and processes mean to all members.
"These lines are vertical, between the Board and its sections, committees, councils and work groups," says Gray. "Importantly, they are also horizontal, ensuring that where similar or related work is being undertaken by other members this is enhanced by being better coordinated and by eliminating duplicative work."
What will governance look like in five years as the College enters the final phase of its 2019-2023 Strategic Plan? The solid foundation built by members of the Governance Committee is key to future governance success. It will be up to the Governance Committee to work over the next five years to ensure the College's governance remains aligned to the ambitions of the Strategic Plan.
"In 2023, I hope the lines of communication within the College will be more robust and that all committees, councils and sections understand the governance structure within which they work and feel supported in the work they do. And that we will have made clearer the opportunities for member participation in College activities and how those who are interested can get involved," says Gray.
"I also hope that greater opportunities will exist for members to develop leadership skills, the College is transparently inclusive in its processes, member value is increased and its international engagement continues to grow. These aspirations require well-functioning organizational governance and my colleagues on the Governance Committee will do our best to rise to the challenge and deliver."
Clinical Topics: Acute Coronary Syndromes, Anticoagulation Management, Arrhythmias and Clinical EP, Cardiac Surgery, Congenital Heart Disease and Pediatric Cardiology, Diabetes and Cardiometabolic Disease, Dyslipidemia, Geriatric Cardiology, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Pericardial Disease, Prevention, Pulmonary Hypertension and Venous Thromboembolism, Sports and Exercise Cardiology, Stable Ischemic Heart Disease, Valvular Heart Disease, Vascular Medicine, Anticoagulation Management and ACS, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Cardiac Surgery and Arrhythmias, Cardiac Surgery and CHD and Pediatrics, Cardiac Surgery and Heart Failure, Cardiac Surgery and SIHD, Cardiac Surgery and VHD, Congenital Heart Disease, CHD and Pediatrics and Arrhythmias, CHD and Pediatrics and Imaging, CHD and Pediatrics and Interventions, CHD and Pediatrics and Prevention, Acute Heart Failure, Pulmonary Hypertension, Interventions and ACS, Interventions and Imaging, Interventions and Structural Heart Disease, Interventions and Vascular Medicine, Angiography, Nuclear Imaging, Hypertension, Sleep Apnea, Sports and Exercise and Congenital Heart Disease and Pediatric Cardiology, Sports and Exercise and ECG and Stress Testing, Sports and Exercise and Imaging, Chronic Angina
Keywords: ACC Publications, Cardiology Magazine, Acute Coronary Syndrome, Anticoagulants, Arrhythmias, Cardiac, Cardiac Surgical Procedures, Metabolic Syndrome, Angina, Stable, Heart Defects, Congenital, Dyslipidemias, Geriatrics, Heart Failure, Angiography, Diagnostic Imaging, Pericarditis, Secondary Prevention, Hypertension, Pulmonary, Sleep Apnea Syndromes, Sports, Angina, Stable, Exercise Test, Heart Valve Diseases, Aneurysm
< Back to Listings