
MAC Attacks: Unusual Complications of Mitral Annular Calcification
Mitral annular calcification (MAC) is common in the setting of chronic kidney disease and aging. Previously presumed "degenerative" in etiology, cardiac/vascular calcification is now understood to be inflammatory, involving osteoblastic transformation of myofibroblasts. Calcified aortic valves may even contain lamellar bone and bone marrow. MAC shares risk factors with atherosclerosis and is associated with cardiovascular events. Interest in MAC has been rising along with transcatheter edge-to-edge repair and transcutaneous mitral valve replacement, as MAC can complicate these procedures (Figure 1).1
Figure 1
Mitral stenosis due to severe MAC is increasingly encountered. As opposed to rheumatic disease, commissural fusion is absent. Instead, a calcium "tunnel" forms at the leaflet bases, which limits valve opening (Video 1). Currently, these patients are treated on a case-by-case basis because valve replacement (surgical or transcutaneous) carries significant risks.
Video 1
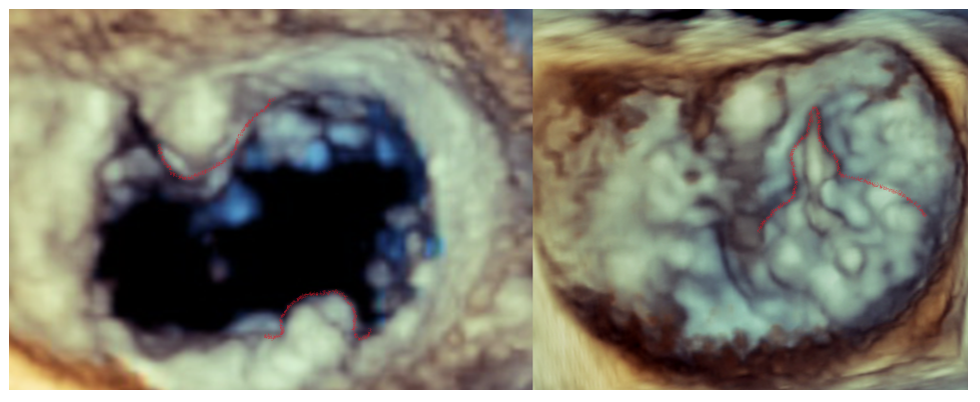
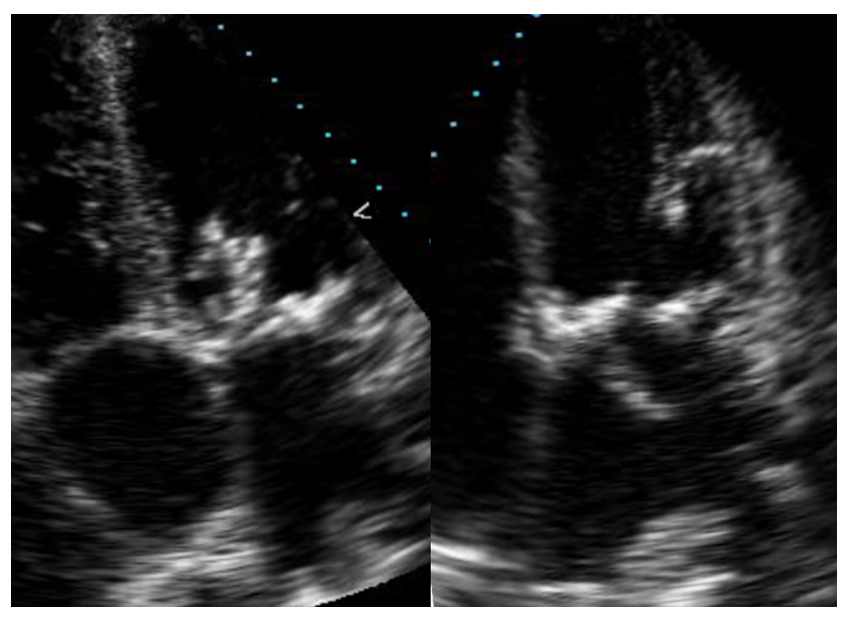
This vignette highlights other less common complications of MAC. Figure 2 is from a patient with end-stage kidney disease who developed MAC that protruded into the left atrium. A calcific projection contacted the anterior mitral leaflet in systole (Videos 2, 3), causing leaflet perforation with both systolic and diastolic flow on color Doppler. One other similar case has been previously reported.2
Figure 2
Video 2

Video 3
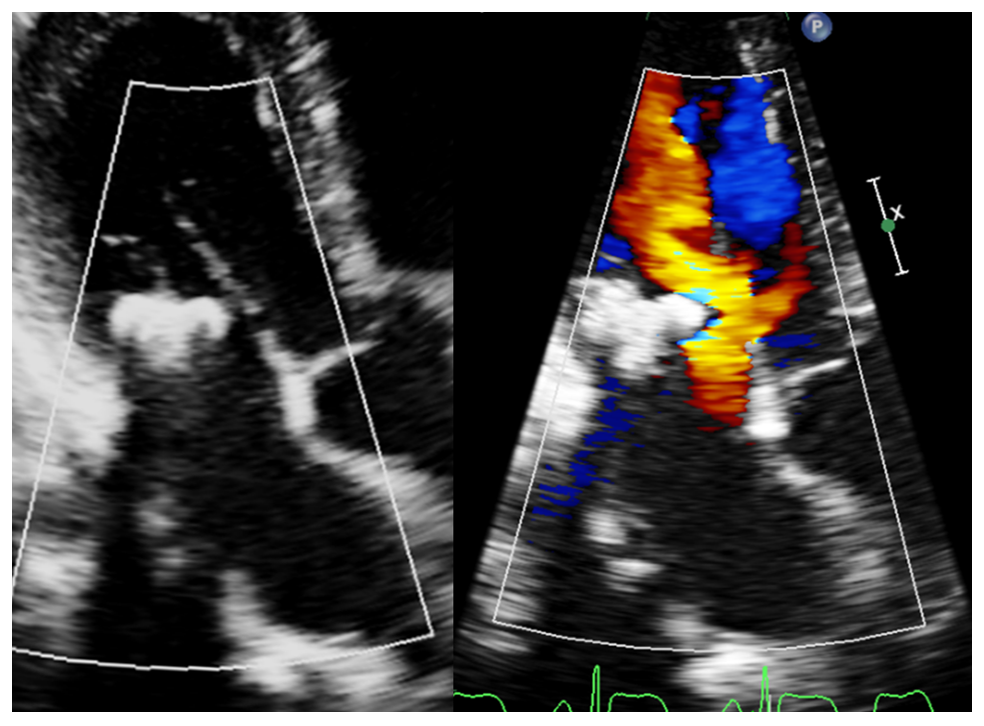
MAC can serve as a nidus for endocarditis (Figure 3). Mechanisms might include alteration of laminar flow over the annulus, MAC-related inflammation, and perhaps erosion of the endocardial surface by the calcium deposits. Bacteriology of MAC-related endocarditis favors Staphylococcus aureus and can produce large vegetations (Video 4). There is also a greater risk of annular perforation than of other types of endocarditis.
Figure 3
Video 4
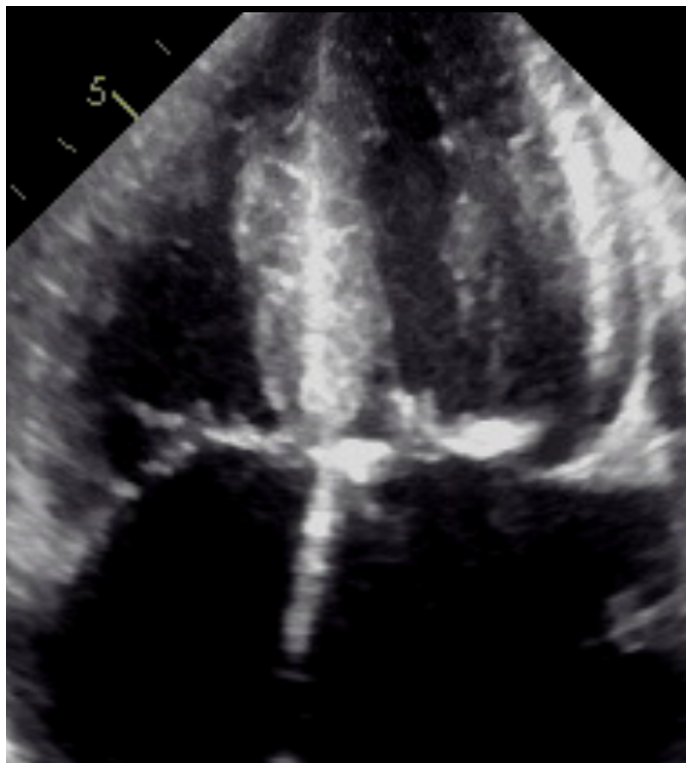
Finally, bulky calcifications can sometimes displace the valve leaflets and their coaptation point toward the ventricular septum. Systolic anterior motion (SAM) and dynamic outflow tract obstruction can result (Figure 4; Video 5).3 These patients tend to have elongated leaflets and small left ventricular cavity size. Associated gradients can be quite high. Subsequent echocardiograms may not show SAM, presumably because of altered hemodynamics.
Figure 4
Video 5
References
- Hatab T, Bou Chaaya RG, Zaid S, et al. Feasibility and outcomes of mitral transcatheter edge-to-edge repair in patients with variable degrees of mitral annular calcification. J Am Heart Assoc 2023;12:[ePub ahead of print].
- Haruki N, Sumi N, Kobara S, et al. Spontaneous mitral valve perforation associated with mitral annular calcification-related calcified amorphous tumor assessed by three-dimensional transesophageal echocardiography. J Med Ultrason (2001) 2020;47:481-2.
- Friend EJ, Wiener PC, Murthy KS, Peterson E, Al-Sudani H, Pressman GS. Systolic anterior motion of the mitral valve in the presence of annular calcification. J Am Soc Echocardiogr 2023;36:421-7.
Clinical Topics: Valvular Heart Disease, Noninvasive Imaging
Keywords: Mitral Valve, Mitral Valve Stenosis, Renal Insufficiency, Chronic, Vascular Calcification, Myofibroblasts