

Feature | Addressing Mitral Regurgitation: Insights From CardioSurve
Transcatheter therapy for repair or replacement of the mitral valve (MV) is transforming the treatment of mitral regurgitation (MR). Along with an expanding evidence base, with perhaps the COAPT results in patients with heart failure and moderate/severe secondary MR being the most recent installment to advance the field, there are numerous efforts to educate cardiovascular professionals. MR is the most common type of moderate or severe heart valve disease among U.S. adults older than 55 years and its prevalence is increasing.
Just a month ago the ACC and the American Association for Thoracic Surgery held a three-day Heart Valve Summit, which included discussion of the latest research on MR, including COAPT and pivotal MR trials ahead, and practical strategies for characterizing and managing MR. Further guidance comes from the 2017 Expert Consensus Decision Pathway on the Management of Mitral Regurgitation, which focuses on the evaluation and management of patients with MR, with an emphasis on 1) clinical assessment; 2) proper identification of the mechanism and etiology of MR; 3) determination of MR severity; 4) assessment of the feasibility of surgical or transcatheter repair in appropriate patients; and 5) indications for referral to a regional comprehensive valve center.
In this fast-changing environment that offers new options for patients, what are the views of cardiovascular professionals about the evaluation and management of MR? A survey of 161 active Fellows of the ACC conducted via ACC's CardioSurve Panel helps to answer this question.
Patient Evaluation
 Click the image above for a larger view.
Click the image above for a larger view.
Each month, about half (48 percent) of the respondents see ≤10 patients with MR, 25 percent see 11-25 patients and 27 percent see ≥26 patients with MR.
Echocardiography is a key tool to evaluate valvular heart disease. Most (79 percent) respondents were low-volume readers of echos (≤25 percent of their time) and only 19 percent were high-volume readers (>25 percent of time).
One of four cardiologists who see MR patients stated a high degree of confidence in using auscultation to detect and characterize MR. A slightly higher proportion (37 percent) of high-volume echo readers expressed a high degree of confidence for using auscultation.
In patients with MR of unknown severity, the parameters typically included in echo reports with a frequency of ≥90 percent include tricuspid regurgitation, left ventricular end systolic dysfunction, MV morphology, Doppler grading of MR severity (semi-qualitative), regional LV wall motion assessment, right ventricular (RV) function and RV systolic pressure. For high-volume echo readers, the top five most frequently reported echo elements are RV systolic pressure, RV size, MV morphology, Doppler grading of MR severity (semi-qualitative) and regional LV wall motion assessment (96-100 percent inclusion).
High-volume echo readers expressed a high level of confidence in determining the mechanism (86 percent) and severity (87 percent) of MR based on echo findings. In contrast, just over two of three of the low-volume echo readers expressed a high level of confidence in determining whether a patient meets the criteria for MR treatment based on echocardiography findings.
One respondent acknowledged, "Mitral regurgitation severity can be challenging by echocardiogram. Look at the left atrial size!"
Another stated that in private practice, it's not practical and it's too time consuming ("that's reality") to do a full diastology exam and every measurement for aortic insufficiency, MR, etc., and that patients are brought back if something needs further definition and the technician is informed of specific measurements to obtain. "Certainly academic centers do everything on everyone (and they can spend an hour per study) and they get more information from the outset. That is an advantage and they have echo cardiology readers that only read echos all day."
Assessment of Outcomes and Referral of Patients
 Click the image above for a larger view.
Click the image above for a larger view.
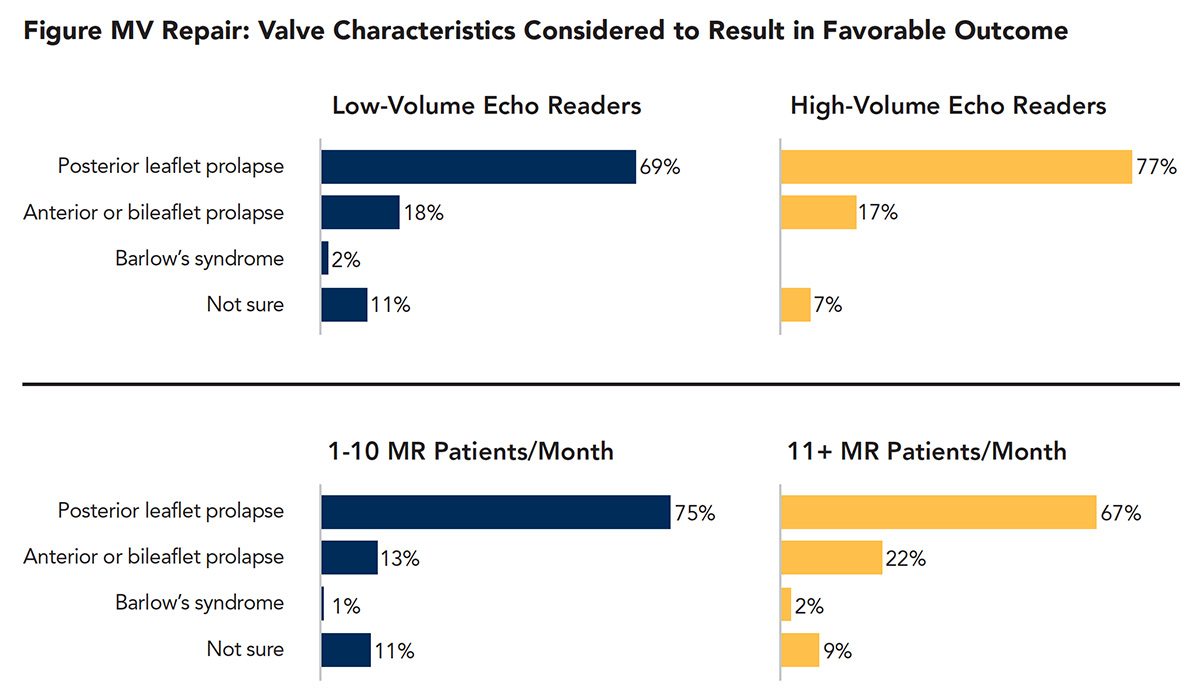
Posterior leaflet prolapse was the valve characteristic considered by seven of 10 respondents to most likely result in a favorable outcome for MV repair, followed by anterior or bileaflet prolapse by 18 percent and Barlow's syndrome by 2 percent; 10 percent were not sure. The responses by audience are detailed in the Figure.
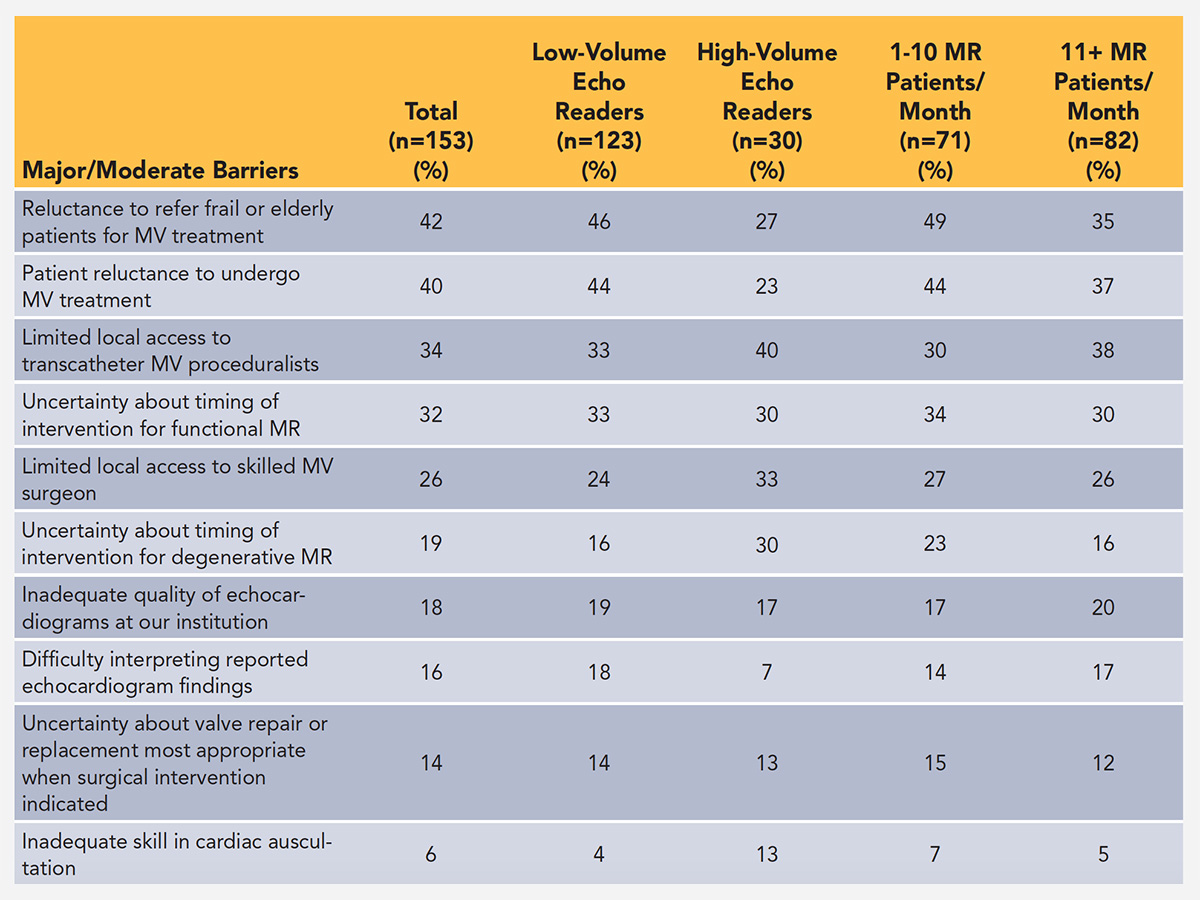
The top barriers that impact the ability of cardiologists to provide optimal care for patients with MR were reluctance to refer frail or elderly patients for MV treatment (42 percent), patient reluctance to undergo MV treatment (40 percent), limited local access to transcatheter mitral valve proceduralists (34 percent) and uncertainty about the timing of intervention for functional MR (32 percent).
The potential barriers to care as viewed by the low- and high-volume echo readers and lower and higher volume of patients are detailed in the Table. Low-volume echo readers (46 percent) and respondents who see ≤10 MR patients per month (49 percent) were more likely to perceive the reluctance to refer frail or elderly patients for MV treatment as a major or moderate barrier, compared with high-volume echo readers (27 percent) or respondents who see ≥11 MR patients per month (35 percent). However, high-volume echo readers (40 percent) and those who see ≥11 MR patients per month (38 percent) were slightly more likely to perceive limited local access to transcatheter MV proceduralists as a major or moderate barrier than were low-volume echo readers (33 percent) or those who see ≤10 MR patients per month (30 percent).
The cardiothoracic surgeon and the patient were the top two influencers on deciding the treatment strategy for patients with an indication for MR treatment, reported by 72 percent and 64 percent, respectively, of respondents. One respondent stated, "Clinical symptoms and response to medical therapy is an important entity in chronic mitral regurgitation that should be considered. Patients understand that better than the presence or characteristic of the murmur emphasis."
On a slightly lower tier of influence were the structural cardiologist (heart valve specialist; 44 percent), cardiovascular team member with the heart team (39 percent) and the cardiac imager (38 percent).
Another respondent, an electrophysiologist, noting it's rare to be the cardiologist who primarily manages valvular disease, refers patients approaching the need for intervention to a "cardiologist with experience in valvular disease but who does not do interventions so I can get a less biased opinion on the timing and choice of intervention."
The need for specialists on both ends of the age spectrum was raised by two respondents. A pediatric cardiologist noted the limited exposure to MV disease requiring intervention in structurally normal four-chamber hearts. Another respondent wished there was a geriatric cardiologist on the local heart team, stating that while what to do technically is often known, "We don't often have or always exercise the wisdom of what should or should not be done."

What is the access for specialists and heart valve centers within 50 miles of their practice? Four of five respondents (82 percent) stated they have a surgeon skilled in MV repair and 72 percent have a surgeon or interventionalist skilled in transcatheter MV procedures. Nearly two of three (64 percent) have a Heart Valve Center of Excellence and about half (49 percent) have a surgeon skilled in MV replacement, but not repair. About half of the cardiologists (53 percent) send their patients with MR who are candidates for valve treatment to a surgeon skilled in MV procedures, while 25 percent send their patients to a Heart Valve Center of Excellence.
What do the respondents say about availability of services? "We have a Valve Center of Excellence within 300 miles. Works well for our patients if needed for mitral valve clip." "I send patients out of town to a skilled robotic MVR surgeon." "I work at the VA [Veterans' Administration] and can refer patients to the heart hospital for mitral valve clipping. For other candidates, I always tell them they should try to get a surgeon who can do mitral valve repair. Usually I do the TEE [transesophageal echocardiogram] and can tell if there is a possibility of repair."
In terms of judging the quality of referral centers, one respondent stated, "Data for surgical volume and outcomes are not available. It's hard to trust non-peer reviewed data from hospitals due to commercial biases." Another noted it'd be helpful to have a list of heart valve centers from ACC, adding "These are usually complex decisions that require input from the treating cardiologist, echocardiographer, structural cardiologist and cardiothoracic surgeon."
"This can be a very frustrating condition to manage. I am always concerned with upfront risk to the patient vs. risk of deterioration later. I am eager to see the outcomes with transcatheter techniques."
Clinical Topics: Arrhythmias and Clinical EP, Cardiac Surgery, Heart Failure and Cardiomyopathies, Noninvasive Imaging, Valvular Heart Disease, Atrial Fibrillation/Supraventricular Arrhythmias, Aortic Surgery, Cardiac Surgery and Arrhythmias, Cardiac Surgery and Heart Failure, Cardiac Surgery and VHD, Acute Heart Failure, Echocardiography/Ultrasound, Mitral Regurgitation
Keywords: ACC Publications, Cardiology Magazine, Aortic Valve Insufficiency, Atrial Fibrillation, Auscultation, Blood Pressure, Echocardiography, Echocardiography, Transesophageal, Heart Failure, Heart Valve Diseases, Mitral Valve, Mitral Valve Prolapse, Mitral Valve Insufficiency, Private Practice, Prolapse, Referral and Consultation, Risk, Surgeons, Surgical Instruments, Thoracic Surgery, Tricuspid Valve Insufficiency, United States Department of Veterans Affairs, Ventricular Function, Right
< Back to Listings