Cover Story | One Size Does Not Fit All: The Role of Sex, Gender, Race and Ethnicity in Cardiovascular Medicine

It's been 17 years since the Institute of Medicine's report on sex-based disparities in health care and 15 years since its similar report on racial disparities.1,2 While there has been some improvement, many of these disparities remain, particularly in cardiovascular disease incidence, prevention, treatment and outcomes.
Blacks have the highest rate of cardiovascular disease in the U.S., with about 47 percent affected. By 2035, that figure is expected to rise to 50 percent. Similar increases will occur in Hispanics, 30 percent of whom had cardiovascular disease in 2015, and in women, in whom the rate of cardiovascular disease is expected to rise from about 41 percent in 2015 to close to 45 percent in 2035.3
Blacks are also two to three times as likely as whites to die from heart disease. And while the overall cardiovascular mortality rate had been falling in recent years (but is now increasing), differences based on race and ethnicity have barely budged.4,5 In addition, while men have always had the lead in terms of cardiovascular rates, women appear to be catching up.3
Indeed, disparities can be found in every major area of cardiovascular medicine:
Primary and secondary prevention. Physicians are less likely to discuss cardiovascular disease risk, perform guideline-directed risk assessments or provide quality preventive care with women.6-8 For instance, women with atherosclerotic cardiovascular disease are less likely to be prescribed lipid-lowering therapies than men or have treatment intensified.9
Risk factors. Black and Hispanic women have the highest rates of obesity in this country, followed by black and Hispanic men.10 Blacks and Hispanics also lead the country in rates of diabetes and hypertension.4 Meanwhile, diabetes and smoking convey a greater risk of cardiovascular disease in women than men.7
Outcomes. Blacks are 33 percent more likely than whites to die of cardiovascular disease in the hospital setting regardless of the quality of care received, while hospitalized women are less likely to receive guideline-directed care for cardiovascular conditions than men, and 25 percent more likely to die if they receive suboptimal care. One study concluded that 69 percent of sex-based disparities in outcomes could be eliminated if women received better quality of care.11
Disease management. There are substantial differences in treatment patterns based on sex and race/ethnicity. For instance, women and blacks are less likely to be referred for cardiac catheterization when presenting with chest pain than men and whites, respectively.12 Another study in a Medicare population found blacks 42 percent less likely to receive ICDs after a myocardial infarction than whites, leading to reduced long-term survival.13

"All members of the cardiovascular team must understand that cardiovascular health outcomes and adherence to treatment plans are greatly influenced by our patient's gender and cultural and spiritual beliefs," says Jennifer H. Mieres, MD, FACC. "These factors also significantly affect disease presentation, risk factors and treatment."
Understanding Disparities
The reasons for sex, gender, race and ethnic disparities are complex. In women, endogenous and exogenous hormones, genetic differences, gender-based misperceptions and a history of excluding women from cardiovascular clinical trials all play a role.7,14,15


"Remember 'My Fair Lady'?" asks Nanette Kass Wenger, MD, MACC. In the play and movie, the protagonist Henry Higgins moans, "Why can't a woman be more like a man?" The same could be said for clinical cardiology, says Wenger. "There are substantial gender differences in pathophysiology, preventive approaches, clinical presentations, management issues and prognosis," between women and men, she adds.
The underlying reasons for race/ethnicity disparities are different but just as complex. The majority are related to the social determinants of health, says Keith C. Ferdinand, MD, FACC. These include socioeconomic status, physical environment, employment status, access to care and social support. Indeed, the social determinants of health make up a larger part of cardiovascular risk factors than nearly any other area of health.16
"These conditions are like a huge cruise ship," says Ferdinand. "They are slow and difficult to turn."
Health care professionals also play a role. For one, studies show low awareness of racial, ethnic or sex-based disparities among cardiovascular professionals.17 In one study, just 35 percent of internal and emergency medicine residents rotating through the cardiac care unit believed that racial disparities existed in this country; after a one-hour educational seminar, however, that number jumped to 85 percent.18 In addition, the nation's workforce of cardiovascular specialists is primarily composed of white men, which may limit their understanding of the unique experiences of women and minorities.19,20
Recognizing sex, gender, racial and ethnic differences in cardiovascular risk factors, disease presentation and treatment response is crucial to improving outcomes in these populations and reducing disparities. The rest of this article highlights specific issues clinicians should be aware of in HF, hypertension, type 2 diabetes (T2D) and atrial fibrillation (AFib) in women, blacks and Hispanics that may affect the quality of care provided and medical outcomes.
Heart Failure
HF in Women
The incidence of HF in women is similar with that in men. However, women tend to be older than men when diagnosed and to have a higher body mass index, hypertension and diabetes. They are also more likely to present with heart failure with preserved ejection fraction (HFpEF).21
HF in Blacks and Hispanics
Blacks and other minorities have a higher risk of HF than whites, with the highest risk in black women. HF in black patients is more likely to stem from hypertension than coronary artery disease, and they are more likely to have HFpEF than whites.22 Blacks are also more likely to achieve a substantial clinical benefit from the use of nitric-oxide-enhancing therapy (isosorbide dinitrate/hydralazine) than whites and other ethnicities.23
In addition, angiotensin-converting enzyme inhibitors are significantly less effective than calcium channel blockers (CCBs) in preventing HF and stroke in blacks with hypertension. Thus, the best initial drug therapy for black patients is thiazide diuretics or CCBs.24
Atrial Fibrillation
 Click the image above for a larger view.
Click the image above for a larger view.
AFib in Women
Women in the U.S. have slightly lower rates of AFib than men, with the Framingham Heart Study finding a lifetime risk at 80 years of 22.7 percent for men and 21.6 percent for women.4 However, women exhibit faster ventricular rates during arrhythmic episodes, longer symptomatic episodes with more frequent occurrences, have a higher risk of stroke and are more likely to die from AFib than men. They also have a lower quality of life.25
Women on warfarin have a higher residual risk of stroke or systemic embolism than men, which could be related to more time spent out of the ideal therapeutic range.26 They also have a higher risk of bleeding.25 However, there are no sex-specific differences in outcomes or bleeding risk between men and women on direct-acting oral anticoagulants (DOACs). In fact, women may have a lower risk of bleeding and ischemic stroke when taking a DOAC than men.26,27
AFib in Blacks and Hispanics
Blacks and Hispanics have a lower incidence of AFib than whites. However, blacks are less likely to be aware they have the condition. They also have a higher prevalence of risk factors for AFib and a much higher overall risk of stroke and stroke-related mortality.28 There is some thought that undetected AFib may contribute to their higher risk of stroke.29
Blacks and Hispanics demonstrate a greater risk of major bleeding with warfarin, as well genetic polymorphisms that may affect warfarin response.30-34 However, there does not appear to be any significant racial or ethnic differences in outcomes or bleeding risk with DOACs.28
Hypertension
 Click the image above for a larger view.
Click the image above for a larger view.
Hypertension in Women
Although rates of hypertension between men and women are similar, hypertension may have a greater impact on a women's cardiovascular risk. One study found that every 10 mm Hg increase in systolic blood pressure in women led to a 10 percent greater risk of cardiovascular disease than in men, although there was no difference in cardiovascular-related mortality.35
Hypertension in Blacks and Hispanics
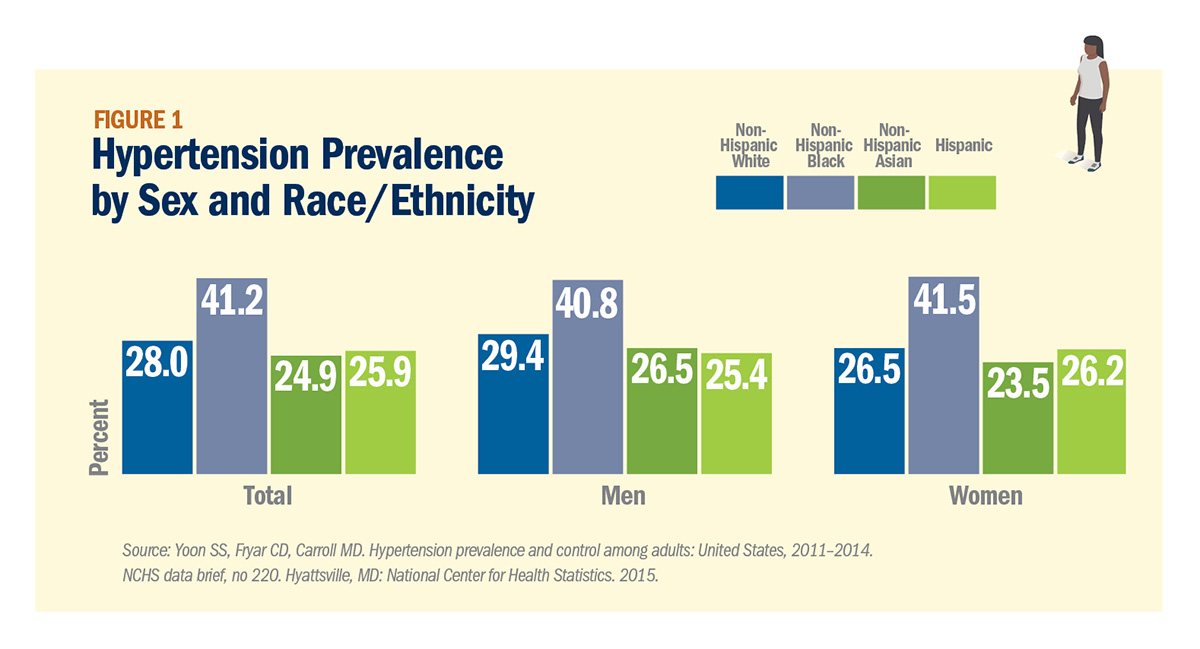
Blacks in the U.S. have the highest rate of hypertension in the world, with a prevalence of 41.2 percent in 2011-2014 compared with 28 percent among whites, 24.9 percent among Asians and 25.9 percent among Hispanics. In addition, blood pressure control rates for blacks with hypertension are lower than other groups, despite higher awareness and treatment rates.4 Blacks are also more salt sensitive, which may be why the DASH diet is particularly effective in this population.24
While numerous factors play into the development of hypertension, one that is unique to blacks, Hispanics and other minorities is racial discrimination.36,37
One reason for poor blood pressure control in blacks may be high rates of nonadherence with antihypertensive medication. Improving adherence, then, should be an important component of antihypertensive management. Improved patient/physician communication, including motivational interviewing, as well reminder systems, pharmacist counseling and automated pill bottles may help.38
Type 2 Diabetes
T2D in Women
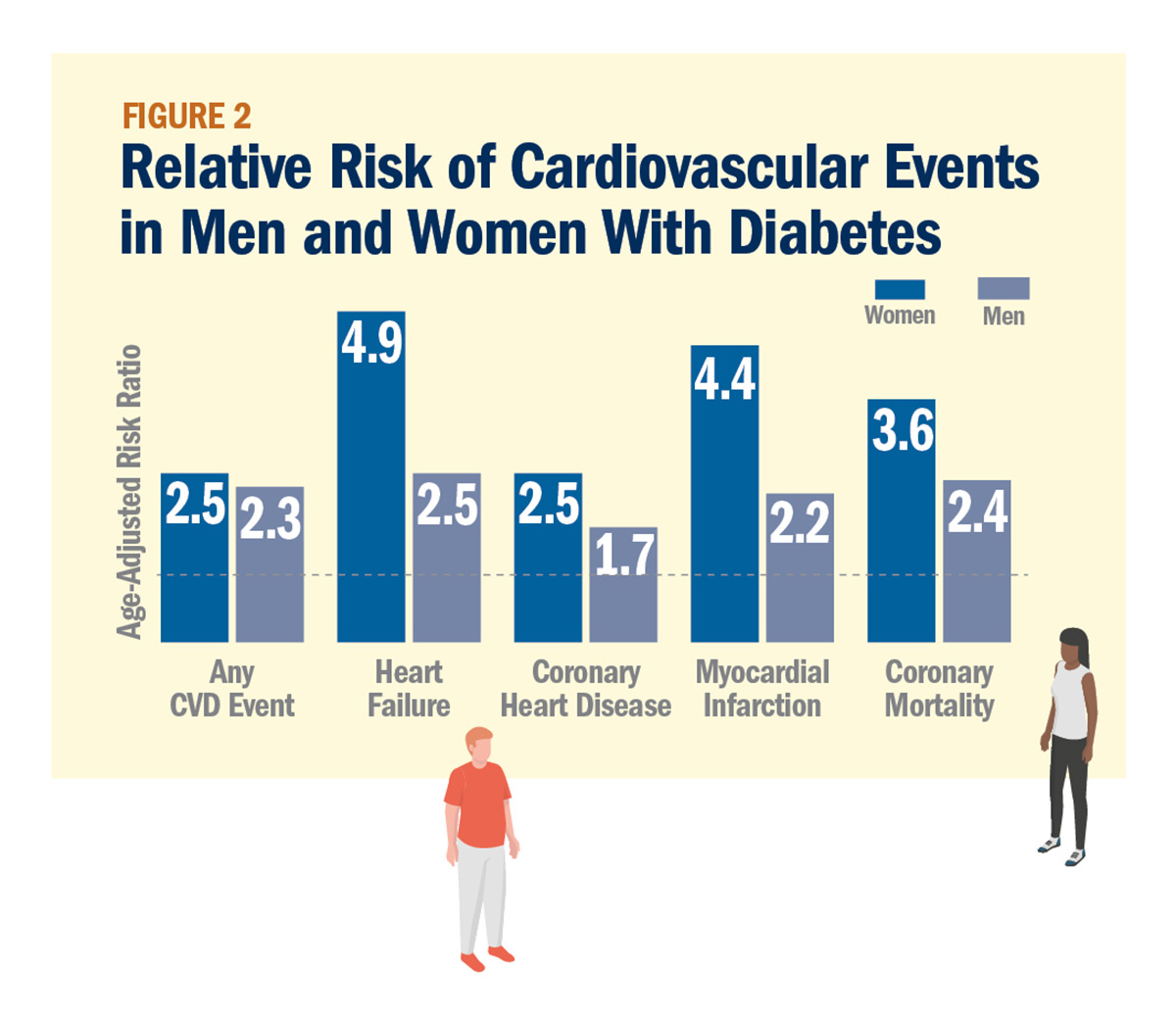
As with hypertension, diabetes in women appears to be a stronger risk factor for cardiovascular disease than in men (Figure 2). One analysis of more than 850,000 people with diabetes found that women with the disease had a 44 percent higher risk of cardiovascular disease and 27 percent higher risk of stroke than men.39
T2D in Blacks and Hispanics
There are significant racial and ethnic disparities in the rate of diabetes in the U.S., with 12.1 percent of Hispanics and 12.7 percent of blacks affected compared with 7.4 percent of whites. The only group with a higher rate is American Indians/Alaskan Natives, at 15.1 percent.40 Blacks and Hispanics typically have poorer glycemic control than whites, which helps explain higher rates of diabetes-related complications such as amputations and end-stage renal disease.41
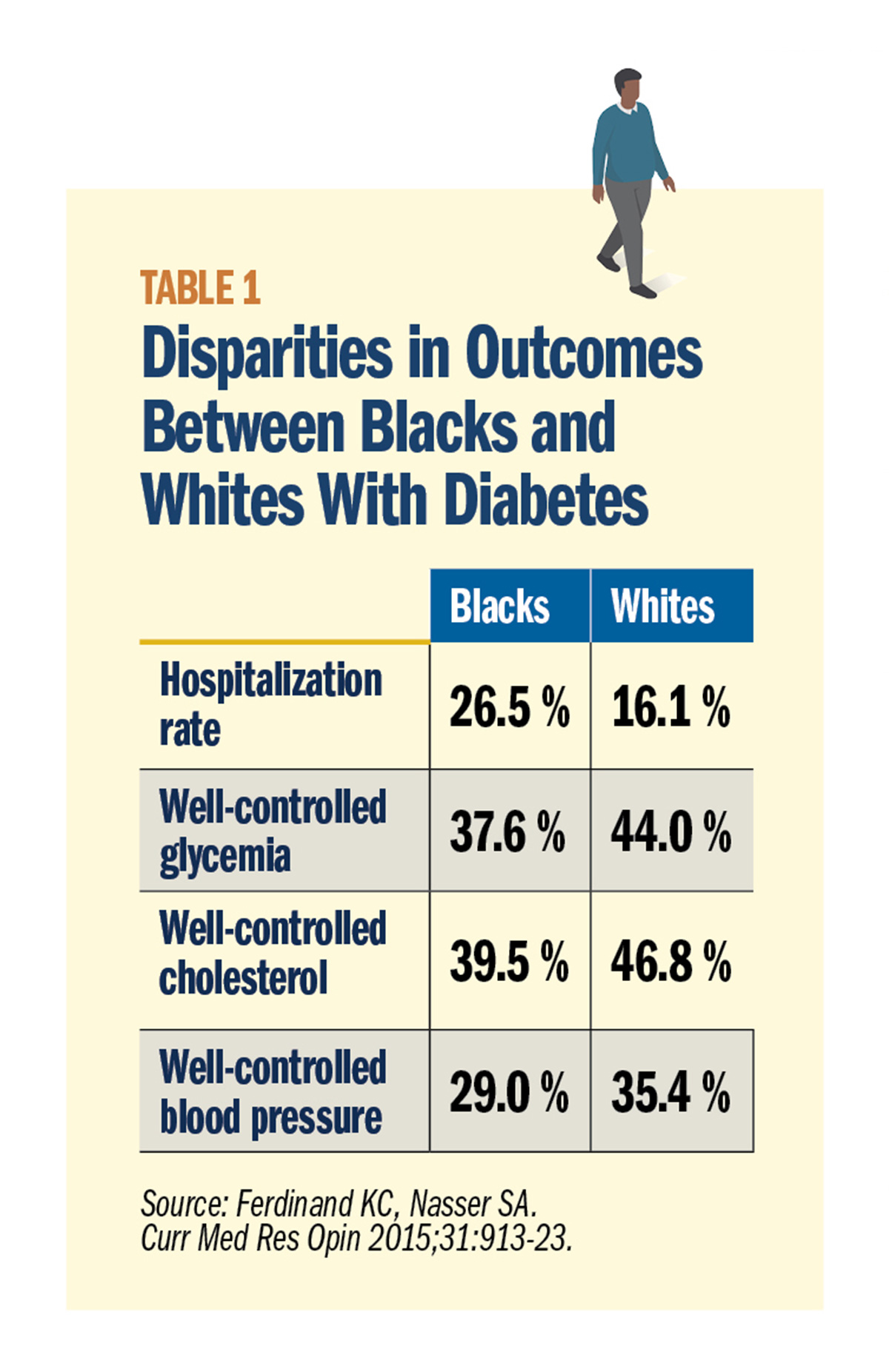
Table 1 highlights other diabetes-related disparities between blacks and whites. When it comes to treatment, there do not appear to be any differences in efficacy or adverse effects with oral and injectable antidiabetic medications used today. However, observational data suggest that clinicians are less likely to intensify treatment in blacks and Hispanics than whites.42 Such clinical inertia can contribute to poorer outcomes.
Conclusion
There are significant disparities in the prevalence, risk factor profile, quality of care and outcomes provided to women and black and Hispanic patients at risk of or with cardiovascular disease.
In the end, these disparities are not the result of individual clinician bias, but reflective of systemic problems within the health care system and in society, says Ferdinand. Nonetheless, it is critically important that cardiovascular professionals are aware of their role in perpetuating disparities, and consider sex, gender, racial and ethnicity in personalizing treatment for their patients.
Pregnancy and Cardiovascular Risk
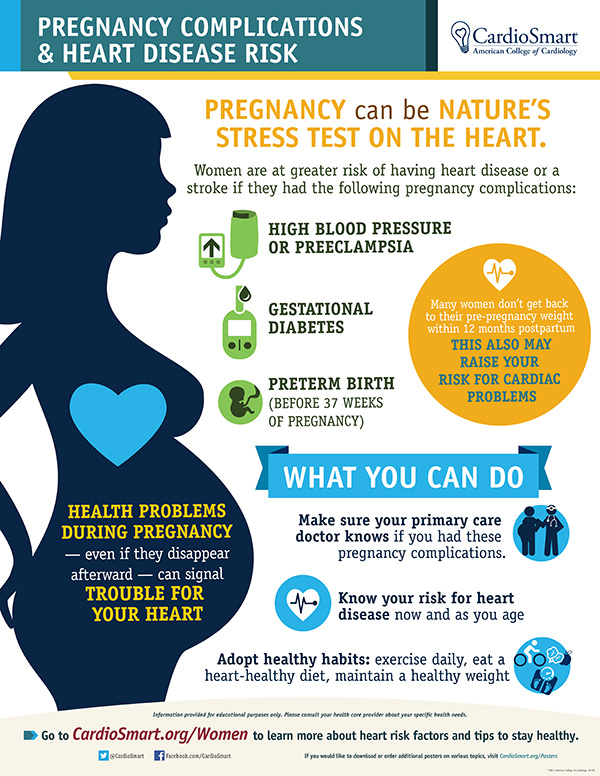
A woman's reproductive history provides important clues to her cardiovascular health. For instance, women with gestational diabetes and preeclampsia have a 26 percent and 31 percent increased 10-year cardiovascular disease risk, respectively. In addition, premature delivery because of preeclampsia increases the risk of cardiovascular disease eightfold vs. women without preeclampsia.43
There is also evidence that delivering a preterm or small-for-gestational-age infant is associated with hospitalization or death from cardiovascular disease later in the mother's life, even after accounting for socioeconomic factors, smoking and pregnancy-related complications.44
Cardiovascular professionals should incorporate pregnancy-related complications into the medical history when assessing cardiovascular risk in women.
Visit CardioSmart.org/Posters to download the pregnancy infographic.
Don't miss November's cover story on gestational cardiovascular disease.
References
- Wizemann TM, Pardue ML. Exploring The Biological Contributions To Human Health: Does Sex Matter? Institute of Medicine;2001. Available here.
- Smedley BD, Stith AY, Nelson AR. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Institute of Medicine;2003. Available here.
- American Heart Association. Cardiovascular Disease: A Costly Burden for America. Projections Through 2035. Available here.
- Benjamin EJ, Virani SS, Callaway CW, et al. Circulation 2018;137:e67-e492.
- Van Dyke M, Greer S, Odom E, et al. MMWR Surveill Summ 2018;67:1-11.
- Bairey Merz CN, Andersen H, Sprague E, et al. J Am Coll Cardiol 2017;70:123-32.
- Bairey Merz CN, Ramineni T, Leong D. Curr Opin Cardiol 2018;33:500-5.
- Mosca L, Linfante AH, Benjamin EJ, et al. Circulation 2005;111:499-510.
- Rodriguez F, Olufade TO, Ramey DR, et al. J Womens Health (Larchmt) 2016;25:697-706.
- Byrd AS, Toth AT, Stanford FC. Curr Obes Rep 2018;7:130-8.
- Li S, Fonarow GC, Mukamal KJ, et al. Circ Cardiovasc Qual Outcomes 2016;9:S36-44.
- Schulman KA, Berlin JA, Harless W, et al. N Engl J Med 1999;340:618-26.
- Groeneveld PW, Heidenreich PA, Garber AM. Circulation 2003;108:286-91.
- Zhao D, Guallar E, Ouyang P, et al. J Am Coll Cardiol 2018;71:2555-66.
- Scott PE, Unger EF, Jenkins MR, et al. J Am Coll Cardiol 2018;71:1960-9.
- Havranek EP, Mujahid MS, Barr DA, et al. Circulation 2015;132:873-98.
- Capers Q, Sharalaya Z. J Racial Ethnic Health Disparities 2014;1:171. Available here.
- Greysen SR, Siegel B, Sears V, et al. J Grad Med Educ 2011;3:417-20.
- Lau ES, Wood MJ. Clin Cardiol 2018;41:264-68.
- Association of American Medical Colleges. Diversity in the Physician Workforce: Facts and Figures 2014. Available here.
- Levinsson A, Dubé M-P, Tardif JC, de Denus S. ESC Heart Fail 2018;5:745-54.
- Gupta DK, Shah AM, Castagno D, et al. JACC Heart Fail 2013;1:156-63.
- Taylor AL, Ziesche S, Yancy C, et al. N Engl J Med 2004;351:2049-57.
- Whelton PK, Carey RM, Aronow WS, et al. J Am Coll Cardiol 2018;71:e127-e248.
- Volgman AS, Manankil MF, Mookherjee D, Trohman RG. Gend Med 2009;6:419-32.
- Ko D, Rahman F, Martins MA, et al. Nat Rev Cardiol 2017;14:113-24.
- Law SWY, Lau WCY, Wong ICK, et al. J Am Coll Cardiol 2018;72:271-82.
- Ferdinand KC, Puckrein GA. J Natl Med Assoc 2015;107:59-67.
- Amponsah MK, Benjamin EJ, Magnani JW. Curr Cardiovasc Risk Rep 2013;7. Available here.
- Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. J Am Coll Cardiol 2007;50:309-15.
- Broderick JP, Brott T, Tomsick T, Huster G, Miller R. N Engl J Med 1992;326:733-6.
- Sacco RL, Boden-Albala B, Gan R, et al. Am J Epidemiol 1998;147:259-68.
- Fang J, Foo SH, Jeng JS, Yip PK, Alderman MH. Ethn Dis 2004;14:378-83.
- Capodanno D, Angiolillo DJ. Thromb Haemost 2010;104:471-84.
- Peters SA, Huxley RR, Woodward M. Stroke 2013;44:2394-2401.
- Brondolo E, Libby DJ, Denton EG, et al. Psychosom Med 2008;70:49-56.
- Williams DR, Mohammed SA. J Behav Med 2009;32:20-47.
- Ferdinand KC, Yadav K, Nasser SA, et al. J Clin Hypertens (Greewich) 2017;19:1015-24.
- Peters SA, Huxley RR, Sattar N, Woodward M. Curr Cardiovasc Risk Rep 2015;9:36.
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017: Estimates of Diabetes and Its Burden in the United States. Available here.
- Ferdinand KC, Nasser SA. Curr Med Res Opin 2015;31:913-23.
- Raebel MA, Ellis JL, Schroeder EB, et al. Pharmacoepidemiol Drug Saf 2014;23:699-710.
- Fraser A, Nelson SM, Macdonald-Wallis C, et al. Circulation 2012;125:1367-80.
- Bonamy AK, Parikh NI, Cnattingius S, Ludvigsson JF, Ingelsson E. Circulation 2011;124:2839-46.
- Brown HL, Warner JJ, Gianos E, et al. Circulation 2018;137:e843-e852.
Clinical Topics: Anticoagulation Management, Arrhythmias and Clinical EP, Cardiovascular Care Team, Dyslipidemia, Heart Failure and Cardiomyopathies, Prevention, Atherosclerotic Disease (CAD/PAD), Anticoagulation Management and Atrial Fibrillation, Atrial Fibrillation/Supraventricular Arrhythmias, Lipid Metabolism, Acute Heart Failure, Hypertension, Smoking
Keywords: ACC Publications, Cardiology Magazine, African Americans, Amputation, Angiotensin-Converting Enzyme Inhibitors, Anticoagulants, Antihypertensive Agents, Atrial Fibrillation, Blood Pressure, Brain Ischemia, Body Mass Index, Calcium Channel Blockers, Cardiac Catheterization, Cardiovascular Diseases, Chest Pain, Coronary Artery Disease, Diabetes Complications, Diabetes Mellitus, Type 2, Diabetes, Gestational, Disease Management, Drug Combinations, Embolism, Emergency Medicine, European Continental Ancestry Group, Factor IX, Gestational Age, Heart Failure, Hispanic Americans, Hospitalization, Hydralazine, Hypertension, Hypoglycemic Agents, Incidence, Indians, North American, Isosorbide Dinitrate, Kidney Failure, Chronic, Lipids, Medicare, Motivational Interviewing, Myocardial Infarction, Nitric Oxide, Obesity, Pharmacists, Polymorphism, Genetic, Pre-Eclampsia, Pregnancy, Prevalence, Prognosis, Quality of Life, Racism, Reminder Systems, Risk Assessment, Reproductive History, Risk Factors, Secondary Prevention, Smoking, Social Class, Social Determinants of Health, Social Support, Socioeconomic Factors, Sodium Chloride Symporter Inhibitors, Specialization, Stroke, Stroke Volume, Treatment Outcome, Warfarin, Sexism
< Back to Listings