

MBA Reflections Part 5: Data-Driven, Values-Based Leadership

"Numbers have an important story to tell. They rely on you to give them a voice." – Stephen Few
What type of leader can I authentically be? This was the first question asked in our longitudinal capstone class. As I thought about how to answer, I didn't have a framework or true idea of how good leadership develops. Now, I think of a leader based on who they are (their values and attributes), and what they do (their literacies and leadership competencies). Values are what we aspire to; our inner compass. Attributes are how we are wired; it is our personality and intelligence. Literacies are our functional knowledge; the core area of skill. Leadership competencies are the behavior and skills needed to lead. An authentic leader is thus able to take numerous and seemingly conflicting facts, and give them a voice consistent with their personal, organizational, and societal values. This is data-driven, values-based leadership.
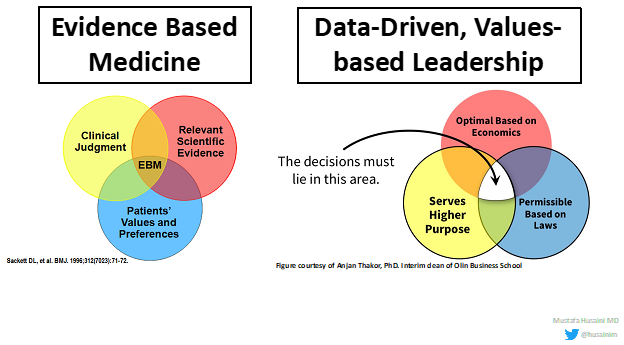
Analogous to how evidence-based medicine lives at the intersection of clinical judgment, relevant scientific evidence, and patients' values and preferences, data-driven values-based leadership lives within a similar intersection (Figure 1). Decisions that connect people to a higher purpose (i.e., values) are related to optimal economics and societal laws (i.e., data).
Another way to think of data-driven, value-based leadership is how values shape the data we collect. Specifically, in medicine, we continually strive for better data to then take the best care of our patients. Striving for better data is reinforced by what we value. For example, data on sex-based differences in athletes will not be available unless we, as a profession, value allocating resources to create this data.
The Social Contract
Another approach to think of data-driven, values-based leadership is through the idea of the social contract. The story of "Pharma Bro" Martin Shkreli exemplifies this. In 2015, his company Turing Pharmaceuticals acquired the U.S. rights to pyrimethamine (Daraprim) for $55 million. He then increased the price per pill from $13.50 to $750.00, mostly based on the idea that the drug was underpriced in the market. He likened it "to an Aston Martin previously being sold at the price of a bicycle." Generally, any business will charge a customer more if it could; in pharmaceutical pricing, the question becomes how much higher the prices could go until the pricing model became unethical. How do you balance reasonable company profits with access to affordable medications?
Steve Miller, MD, the chief medical officer of St. Louis based Express Scripts, a pharmacy benefit manager, describes the social contract as a form of data-driven, values-based leadership:
"There is an unspoken social contract in our country where we permit reasonable profits for pharmaceutical companies as long as those products spur additional innovation and maintain drug affordability and access – especially for a medication like Daraprim which is on the World Health Organization list of Essential Medications. When manufacturers act as Turning has, they have broken the social contract with both patients and the country. And in doing so, they are essentially begging the federal government to step in and implement price controls, an act that would surely erode pharmaceutical innovation in the U.S. and around the globe."
While some may state that Shkreli is not a physician and thus does not have the same ethical standards, there are numerous violations of the social contract in cardiology. A work RVU model creates a "kill-what-you-eat" mentality and moral hazard which has led to gaming, upcoding, and fraud. It is thus imperative to evaluate if our individual decisions are consistent with the social contract and data-driven, values-based leadership.
High-Value Care
As physicians, we need to be conscientious of the care that we provide and the value that our time provides to our patients. In business, we often define value by price. The value to a producer of a good or service is the profit over their cost of production while the value to a consumer is the extra benefits they derive above the price paid. In health care, there are more inputs to consider; in equation form, value = (quality + safety + patient experience) / cost. A more stringent definition of value in health care is that of high-value care.
Is This Solving the Correct Problem?
In MBA Reflections Part 1, I stated that the point of business is to solve a problem and retain an ethical compass. In health care, numerous initiatives, changes to workflow and rules are often implemented without asking if this is solving the correct problem. This series of events normally unfolds because the correct question was not asked. As future leaders, we need to ensure that we utilize a data-driven, values-based approach to avoid moral licensing and virtue signaling and ask the correct questions to then solve the correct problems. This is how we improve and move our field into the future.
References:
- Bodhanwala S, Bothra A. "Turing Pharmaceuticals: The Ethics of Drug Pricing" Ivey Publishing Nov 8th, 2017.
- McNeely CA, Brown DL. "Gaming, Upcoding, Fraud, and the Stubborn Persistence of Unstable Angina" JAMA Intern Med. 2019;179(2):261-263.
This article was authored by Mustafa Husaini, MBA, MD, FACC, an assistant professor at Washington University in St. Louis with editorial assistance by Mohamed Esmail, CFP. Husaini graduated from the executive MBA program at Olin Business school within Washington University in St. Louis and is a member of ACC's Sports and Exercise Cardiology and CV Management Section Leadership Councils.
This article is in memory of his daughter, Aliza, who was born at the start of his MBA and died a few months before graduation. Social Media: @husainim.
Read more from the series here: Part 1, Part 2, Part 3, Part 4.
This content was developed independently from the content developed for ACC.org. This content was not reviewed by the American College of Cardiology (ACC) for medical accuracy and the content is provided on an "as is" basis. Inclusion on ACC.org does not constitute a guarantee or endorsement by the ACC and ACC makes no warranty that the content is accurate, complete or error-free. The content is not a substitute for personalized medical advice and is not intended to be used as the sole basis for making individualized medical or health-related decisions. Statements or opinions expressed in this content reflect the views of the authors and do not reflect the official policy of ACC.