Focus on EP | We Have Global Health. Why Not Global EP Too?

The field of electrophysiology (EP) has made important advances in recent decades. Yet, the exponential growth has not been equally distributed around the world. Essentially these great advances are all concentrated within big cities and developed countries.
EP procedures can have a great impact on our patients' lives – changing the course of their disease and for some even leading to a cure. Yes, we can cure diseases in EP, and only a few subspecialties can say this! EP has become an important and crucial part of our cardiology armamentarium.
As a foreign medical graduate, trained in the U.S., it's hard for me to ignore these disparities in care. We have a lot of communities without access to adequate care and treatment, and people with treatable arrhythmias who learn how to live with it only because they don't have any other option. Just like there are people with an aborted sudden cardiac death without access to an ICD. I found I couldn't simply continue along the path of research and working in the lab that I was on, and ignore these realities.
Now, I serve on missions to my home country of the Dominican Republic, in addition to my work at the University of Virginia (UVA).
During my education and training journey, I was very fortunate to meet cardiologists serving on a mission in the Dominican Republic through the UVA Cardiovascular Global Health Program. Founded more than a decade ago by Scott Lim, MD, the program works to provide free heart valve screenings and lifesaving cardiac interventions, such as mitral balloon valvuloplasty, transcatheter aortic valve replacement and open heart surgeries, to the underserved population in the Dominican Republic.
When I was just 21 years old, during my last year of medical training in the Dominican Republic, I assisted cardiologists who were on a mission there. I was responsible for selecting and prepping the patients for the procedures. Then I worked with them over the years on many missions to screen the population and provide essential treatment.
Why did I become a cardiologist? Why did I have a goal of being one in the U.S.? I wanted to be more like Lim and others who I worked with on these missions who became role models for me: Pedro E. Urena, MD, FACC; Angela Taylor, MD, MS; Michael Ragosta, MD, FACC; John M. Dent, MD, FACC; and Robert W. Battle, MD, FACC.
They were such a true inspiration for me that after I completed my residency training in New York, I went to the UVA, where they all work, for my fellowship training in cardiology and EP. I continue working there as an adjunct faculty member.
Regálame un Latido: Our Device Mission

Recently, we were inspired to create a device mission to complement our interventional and structural missions. An increase in the prevalence of ischemic cardiomyopathy, hypertensive cardiomyopathy and nonischemic cardiomyopathy became apparent to us over the least three years of our valve missions.
The systolic heart failure resulting from this cardiomyopathy has placed these patients at risk for sudden cardiac death. But the patients we're screening live below the poverty line with limited access to health care, making the cost of a defibrillator prohibitive. Furthermore, the health care system in the Dominican Republic does not cover this lifesaving treatment, not even for secondary prevention.
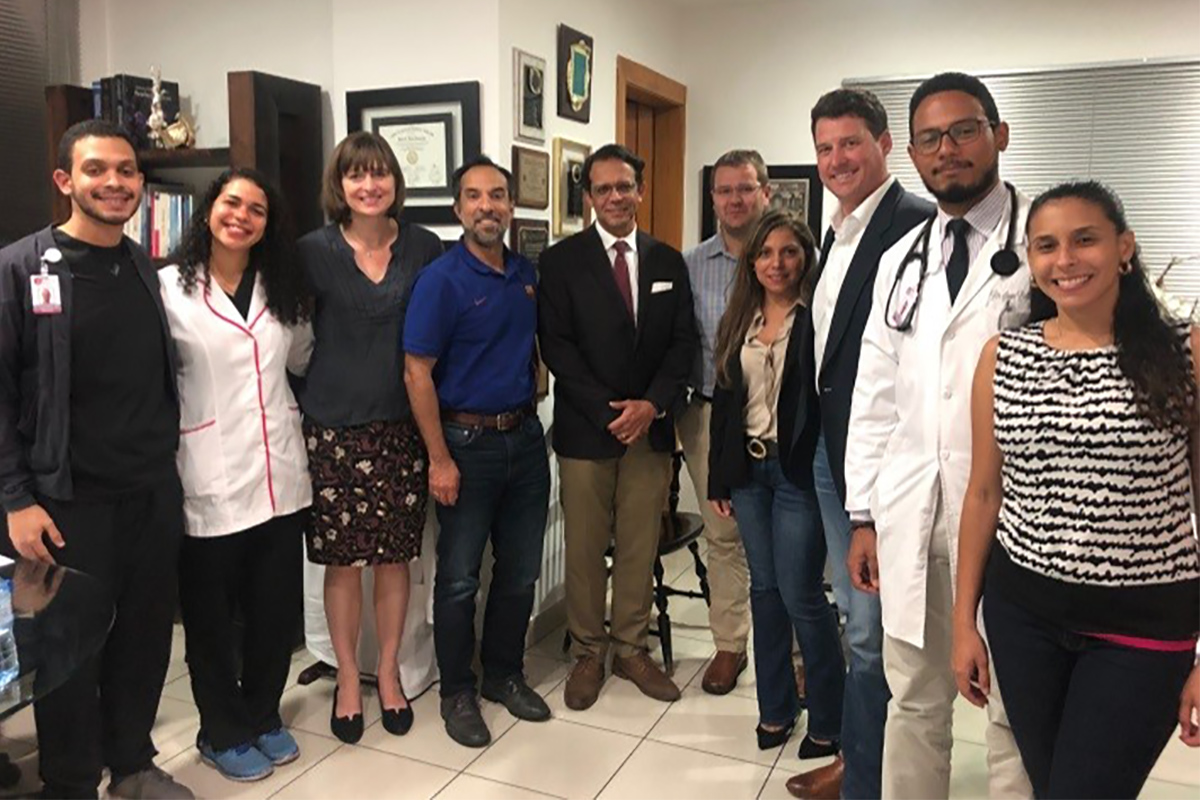
For this mission, we joined forces with Boston Scientific and Medtronic and had support from the UVA Cardiovascular Global Health Program and local support from the Heart Care Dominicana Foundation. Together this created a unique team with a common vision and purpose: help, teach and contribute.
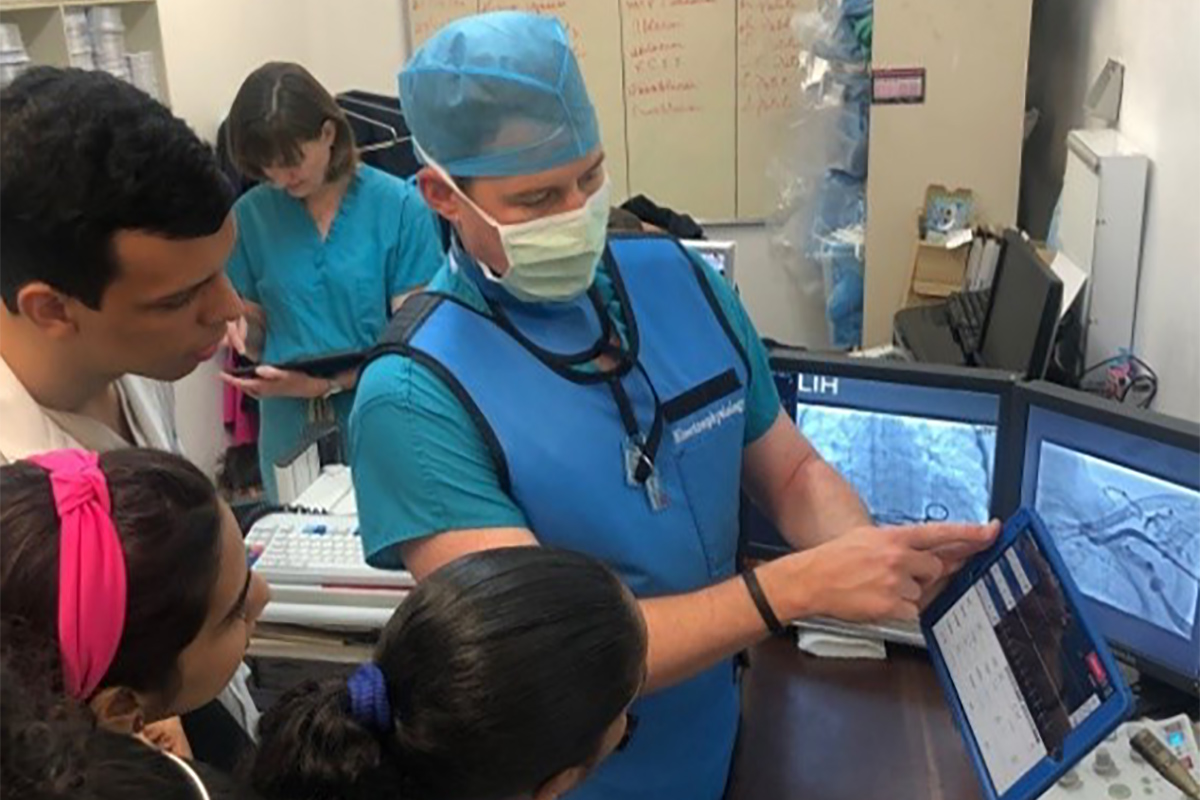
Another important part of the mission was to provide education to Dominican doctors, staff and students. The students played a key role in this mission, responsible for the pre- and postprocedure care of our patients. They were involved from day one to discharge (just like I was 10 years ago).
On the first day, Dominican doctors (pasantes) presented the cases to the team: Urena, president of Heart Care Dominica Foundation; Mason, Rohit Malhotra, MD, FACC, director of cardiovascular/arrhythmia outpatient clinics at UVA; Trip Walker from Medtronic, and two senior EP fellows at that time, Alan Johnson, MD, FACC, and me. We discussed indications, procedure type and coordinated the plan.
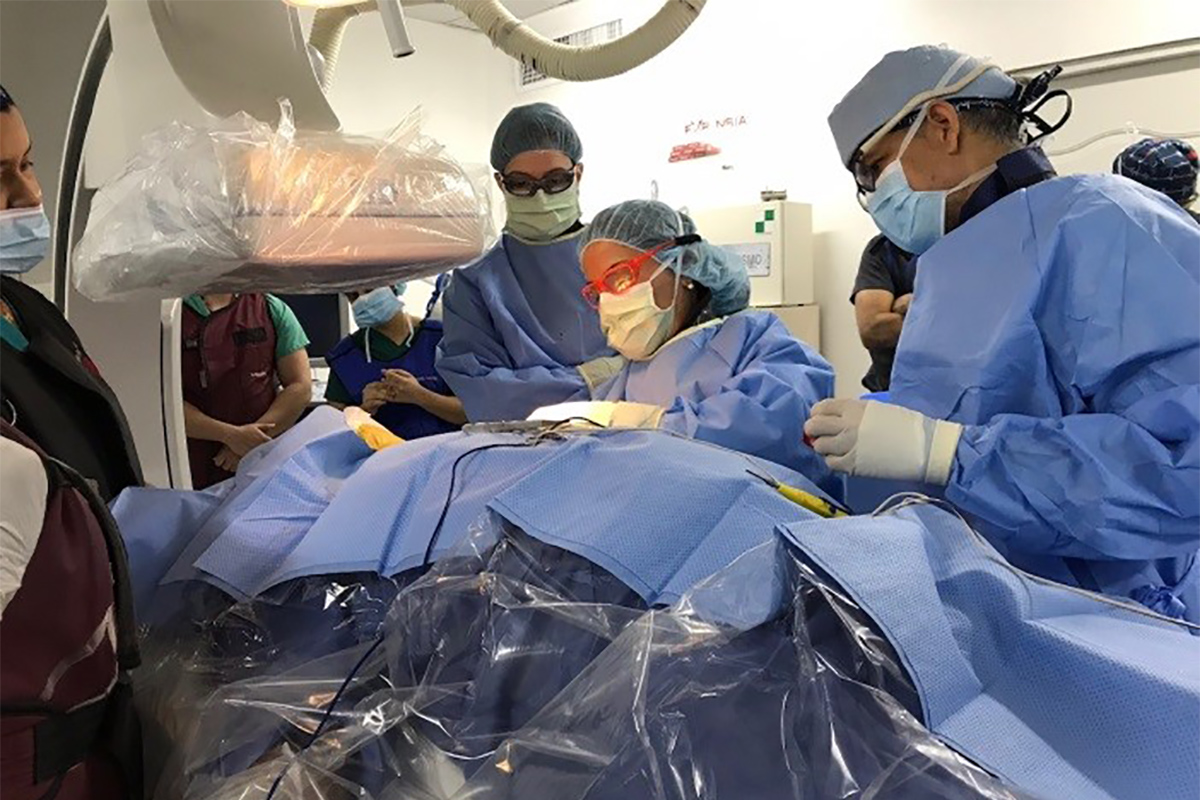
On the second day, we conducted Grand Rounds at Universidad Iberoamericana UNIBE. Then on the third and fourth days, we implanted ICDs. Although our plan was to implant 10 ICDs, one patient on the waiting list died before our mission and another patient was in decompensated heart failure and needed further optimization. Among the eight patients who received an ICD, there have been no complications, either during the cases or during follow-up. Our local counterparts in the Dominican Republic are now following the patients.
The gratitude of our patients and their families wipes away all difficulties and fuels our soul in a very unique way that's hard to describe or compare. We learned more about life than what we gave to them. And for us, this is just the beginning of a longstanding relationship and mentorship. Our goal is to provide education and support, creating a bidirectional relationship where our students can benefit, creating opportunities for future learning and educational exchange – all while we help patients in need.
Global EP?
This is a simple way to prove that Global EP is possible. It confirms each of us can make great contributions if we work together as a team with the common purpose of helping others and remain sensitive to the rest of the world, keeping in touch with reality and to what is happening around us.
It is time to expand EP worldwide, to disseminate the knowledge and the technology, and to educate and train. The world demands more from us. As a doctor it is not enough to take care of an individual patient. We must think globally! We need to be better advocates for the rest of the world, to use our voices to create opportunities and provide them with the tools. These communities have what is needed the most: the human resource!
They have great and talented doctors. They just need an equal distribution and access to new technologies which will, without a doubt, allow them to excel. This reality is not unique for the Dominican Republic; it's similar with many other countries in Latin America, Africa and Asia.
The question now is this: Are you willing to become a global doctor? Are you willing to be part of global EP? #GlobalEPEEPS






This article was authored by Eliany Mejia-Lopez, MD, FACC, cardiac electrophysiologist and adjunctive faculty at UVA, in Charlottesville, VA, and cardiac electrophysiologist at MELOSA Clinica Brugal and Medicina Cardiovascular Asociada, in Santo Domingo, Dominican Republic.
She extends a special thank you to the UVA, which sponsored and mentored her for the creation of this mission. She also expresses her appreciation to the UVA Cardiovascular Global Health Program, especially Dr. Lim and Kimberly Chadwell, MD, and the Heart Care Dominicana Foundation and Dr. Urena, who provided all the local support. And a very special thank you to the great team who volunteer their time and effort to make this possible: Dr. Mason, Dr. Malhotra, Dr. Johnson, Jason Rupp and Trip Walker.
Clinical Topics: Arrhythmias and Clinical EP, Cardiac Surgery, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Prevention, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Cardiac Surgery and Arrhythmias, Cardiac Surgery and Heart Failure, Acute Heart Failure, Chronic Heart Failure
Keywords: ACC Publications, Cardiology Magazine, Foreign Medical Graduates, Fellowships and Scholarships, Developed Countries, Vulnerable Populations, Internship and Residency, Teaching Rounds, Transcatheter Aortic Valve Replacement, Heart Failure, Systolic, Mentors, Secondary Prevention, Balloon Valvuloplasty, Follow-Up Studies, Defibrillators, Implantable, Death, Sudden, Cardiac, Arrhythmias, Cardiac, Cardiomyopathies, Heart Valves, Electrophysiology, Health Services Accessibility, Ambulatory Care Facilities
< Back to Listings