Feature | Cutting-Edge Structural Interventions: The BASILICA Procedure
Transcatheter aortic valve replacement (TAVR) has important potential complications, but arguably the most feared is acute coronary occlusion due to aortic leaflet obstruction. Coronary obstruction is rare following TAVR, with a reported incidence of <1 percent.1
This low incidence is largely attributable to meticulous preprocedural computed tomography (CT) planning. Nonetheless, patients are still either referred for SAVR or treated palliatively because of the possibility of acute coronary occlusion.
Until recently, prophylactic "snorkel" stenting was the only available technique to mitigate the risk of coronary obstruction. While effective, this technique is inherently limited by entrapment of the stent by the transcatheter heart valve (THV), the need for lifelong dual antiplatelet therapy, and the potential need to deploy an unnecessary stent if coronary obstruction did not occur but the positioning of the THV pinned the stent in the coronary ostium.2
BASILICA (bioprosthetic or native aortic scallop intentional laceration to prevent iatrogenic coronary artery obstruction) during TAVR is a novel transcatheter electrosurgical technique developed to avoid coronary obstruction after TAVR.
The concept is simple: using an electrified wire, the left or right aortic leaflet is traversed and lacerated from its base to its free edge to produce a V-shaped splayed leaflet. This allows for flow of blood through the laceration into the coronary sinus and coronary artery ostium post TAVR.
Originally used on a compassionate basis, the BASILICA technique has now been systematically studied in a prospective, multicenter, single-arm, NIH-sponsored investigational device exemption trial. Of the 30 patients in the trial, a solo-BASILICA was attempted in 23 and a doppio-BASILICA was attempted in seven. Traversal and laceration attempts were successful in 95 percent of patients with 100 percent freedom from coronary obstruction after TAVR.3
Since completion of the trial, the BASILICA technique has been performed over 100 times worldwide to prevent coronary obstruction. With established efficacy and an acceptable safety profile, the question remains: who should undergo BASILICA?
Our practice at Emory starts with a careful assessment of the preprocedural CT. Full details are available in a state-of-the-art review recently published in JACC: Cardiovascular Interventions.2

In cases of valve-in-valve (ViV) TAVR, a virtual cylinder with a diameter of the planned TAVR valve is positioned inside the existing surgical bioprosthetic valve using rotational tools to align the cylinder within the bioprosthetic valve posts at all levels. Both coronary ostia are assessed independently for occlusion of the ostia (true coronary obstruction) and sequestration or effacement of the coronary sinus.
First, a qualitative assessment is performed to determine if the existing bioprosthetic valve leaflets are higher than the coronary ostia and if the leaflets reach the level of the sinotubular junction (STJ). A valve-to-coronary (VTC) distance is measured in two perpendicular planes from the simulated cylinder to the point a stent would be deployed if treating ostial coronary atherosclerosis.
In cases where the bioprosthetic surgical valve reaches the sinotubular junction, similar measurements are performed from the simulated cylinder to the narrowest portion of the sinotubular junction. Based on data from the Valve-in-Valve International Data (VIVID) registry, VTC distances <4 mm are deemed to be at intermediate risk and VTC distances <3 mm are deemed to be at high risk.4
We have extrapolated these data to risk assessment at the level of the STJ, but this remains an area of uncertainty given the lack of data on the minimal area required for sufficient coronary blood flow and the flow of blood between coronary sinuses.
Analysis is more difficult in cases of native aortic valve stenosis as leaflet motion is unpredictable post THV deployment. The Emory practice again starts with a qualitative assessment of leaflet length in relationship to the coronary ostium. We begin to consider BASILICA in all cases in which:
- The bottom of the coronary ostium is <10 mm from the annular plane
- The leaflet could reach/cover a significant portion of the coronary ostium
- Long leaflets could reach the STJ. We again simulate THV deployment in the CT scan using a virtual cylinder, and consider patients with a VTC distance <4 mm as intermediate risk and VTC distances <3 mm as high risk for coronary obstruction
Data from our ongoing Coronary Obstruction Risk Assessment (COBRA-TAVR) registry will be presented at TCT 2019 to better define the population with native aortic stenosis likely to benefit from BASILICA.
Valve selection is determined with an emphasis on the risk for "skirt" obstruction.2 In cases of both ViV or native aortic stenosis, coronary obstruction can occur if the THV skirt placement obstructs blood flow into the coronary ostia or STJ.
For the BASILICA procedure itself, dedicated catheters that match the geometric requirements to engage aortic cusp hinge points are now available, and have significantly decreased procedural complexity and time.5
In addition to preventing coronary obstruction, extensive study is underway to determine the impact of BASILICA on flow patterns and washout of the coronary sinuses. Limitations of the technique continue to be the lack of a dedicated laceration system device, diffusely calcified leaflets that prohibit traversal, inability to overcome an obstructive leaflet mass, and skirt obstruction.
Proctorship is currently offered by both Edwards Lifesciences and Medtronic as well as reverse proctorship at the Emory Structural Heart and Valve Center.
While early data are promising, further large-scale study is warranted to better define the clinical outcomes of BASILICA in routine clinical practice. There are plans to begin an international BASILICA registry before the end of 2019.
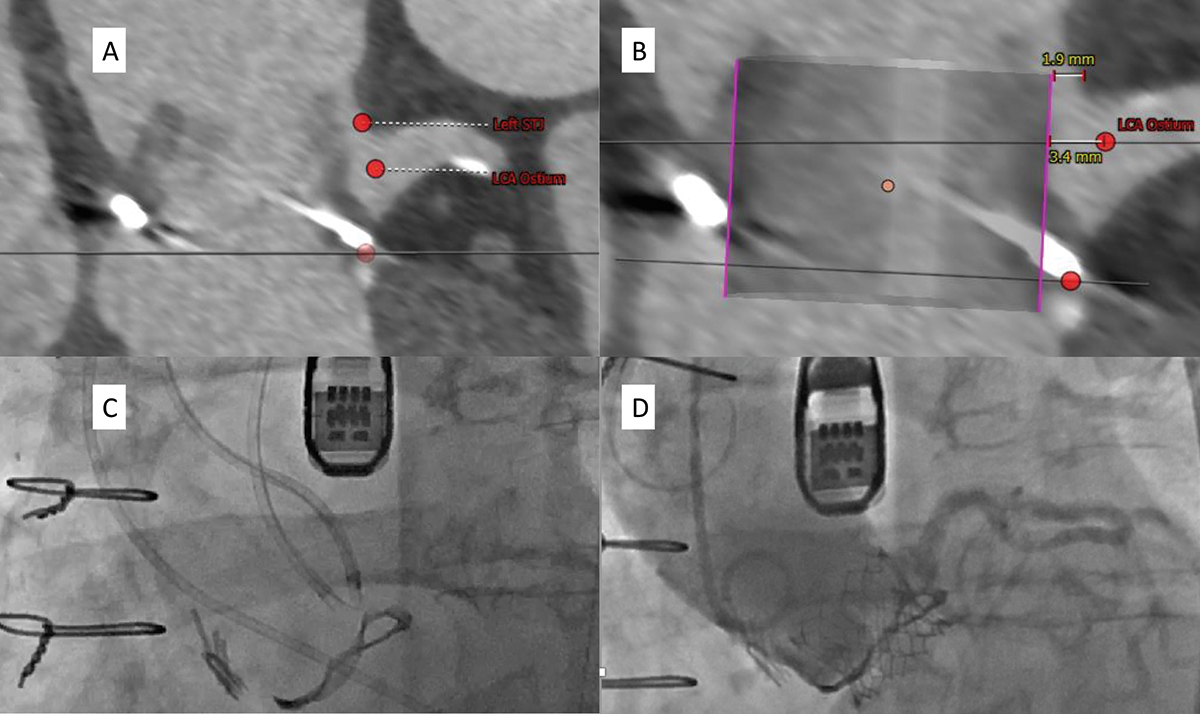
BASILICA Analysis and Laceration A) Note leaflet height is above the coronary ostium and reaches the STJ. B) Both VTC and VTSTJ are <4 mm placing patient at high risk for coronary obstruction. C) BASILICA catheters in place prior to laceration. D) Post deployment angiogram with patent left anterior descending flow.
This article was authored by John Lisko, MD, MPH, a Fellow-in-Training at the Emory Structural Heart and Valve Center in Atlanta, GA.
References
- Ribeiro HB, Webb JG, Makkar RR, et al. J Am Coll Cardiol 2013;62:1552-62.
- Lederman RJ, Babaliaros VC, Rogers T, et al. JACC Cardiovasc Interv 2019;12:1197-1216.
- Khan JM, Greenbaum AB, Babaliaros VC, et al. JACC Cardiovasc Interv 2019;12:1240-52.
- Dvir D, Leipsic J, Blanke P, et al. Circ Cardiovasc Interv 2015;8(1). pii: e002079.
- Lisko JC, Babaliaros VC, Lederman RJ, et al. Cardiovasc Revasc Med 2019;June 6:[Epub ahead of print].
Clinical Topics: Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Valvular Heart Disease, Atherosclerotic Disease (CAD/PAD), Aortic Surgery, Cardiac Surgery and VHD, Interventions and Coronary Artery Disease, Interventions and Imaging, Interventions and Structural Heart Disease, Computed Tomography, Nuclear Imaging
Keywords: ACC Publications, Cardiology Magazine, Transcatheter Aortic Valve Replacement, Coronary Artery Disease, Coronary Occlusion, Incidence, Coronary Sinus, Prospective Studies, Lacerations, Aortic Valve Stenosis, Aortic Valve, Heart Valve Prosthesis, Iatrogenic Disease, Registries, Tomography, X-Ray Computed, Electrosurgery, Surgical Instruments, Risk Assessment, Pectinidae, Tomography, Stents
< Back to Listings