Peripheral Matters | Axillary Artery: Alternate Access for Large Bore Interventional Procedures
 Click image for a larger view.
Click image for a larger view.
The common femoral artery remains the vascular access site of choice in the U.S. for large bore interventional procedures requiring mechanical circulatory support (MCS) and for transcatheter aortic valve replacement (TAVR).1,2 However, the size of the iliac and common femoral arteries varies greatly depending on patient size, comorbidities and gender. Additionally, their caliber may be severely diminished by atherosclerosis and their geometry altered by tortuosity.3,4 As such, the axillary artery has emerged as a viable and safe alternative for large bore arterial access.
Burden of PAD in Patients Referred to Cath Lab
Both peripheral arterial disease (PAD) and coronary artery disease (CAD) have similar risk factors. Thus, it is common to encounter the challenge of treating structural or complex coronary patients with significant concomitant PAD.5-7 Small caliber common femoral and iliac arteries with severe PAD significantly increase the risk for vascular complications. This risk increases greatly when the larger bore sheaths are used.8-11
Feasibility of Axillary Access for Large Bore Sheath
The axillary artery has emerged as a feasible and safe alternative access for delivering large bore sheaths in TAVR or MCS. Although smaller than the common femoral artery, the axillary artery is an acceptable alternative access site for large bore sheaths in the presence of severe PAD in large part due to a low incidence of obstructive atherosclerosis involving this vessel.12,13 Most TAVR and MCS sheaths require a single arterial access for 13 to 16 French sheaths. In a retrospective analysis of 110 CT scans done at a single institution, the mean diameter of the axillary artery was 6.38 mm on the right and 6.52 mm on the left. The axillary arteries demonstrated substantially lower rates of stenosis and of calcification compared with the iliofemoral arteries.14 In 208 patients who underwent routine CT scan for a TAVR procedure, minimal luminal diameters for the axillary arteries and iliofemoral arteries were 6.0±1.1 mm and 6.6±1.8 mm, respectively.15 These findings support the use of the axillary artery for large bore sheaths and has been used for TAVR and MCS devices in patients with severe PAD.12,16-19
Indications for Axillary Access
For patients with severe PAD or those with small caliber iliac and/or femoral arteries (<5 mm), the axillary artery is a viable alternative. Similarly, patients with severe extremely tortuous vessels or with heavy calcification should be considered candidates for axillary artery access. In rare cases, patients who have had an endovascular aortic repair should be considered. Another concern arises when MCS devices are used for prolonged recovery or as a bridge to therapy. When placed via the femoral approach, persistent bed rest is required, which limits ambulation and rehabilitation. However, axillary access allows the patient to ambulate and sit in a chair without limitation, which is an important advantage. Further, in cases with a long dwell time, the axillary approach is considered less prone to infection. Both the left and right axillary arteries have been used for TAVR and MCS devices.12,16-19
Anatomical Landmarks for Accessing the Axillary Artery
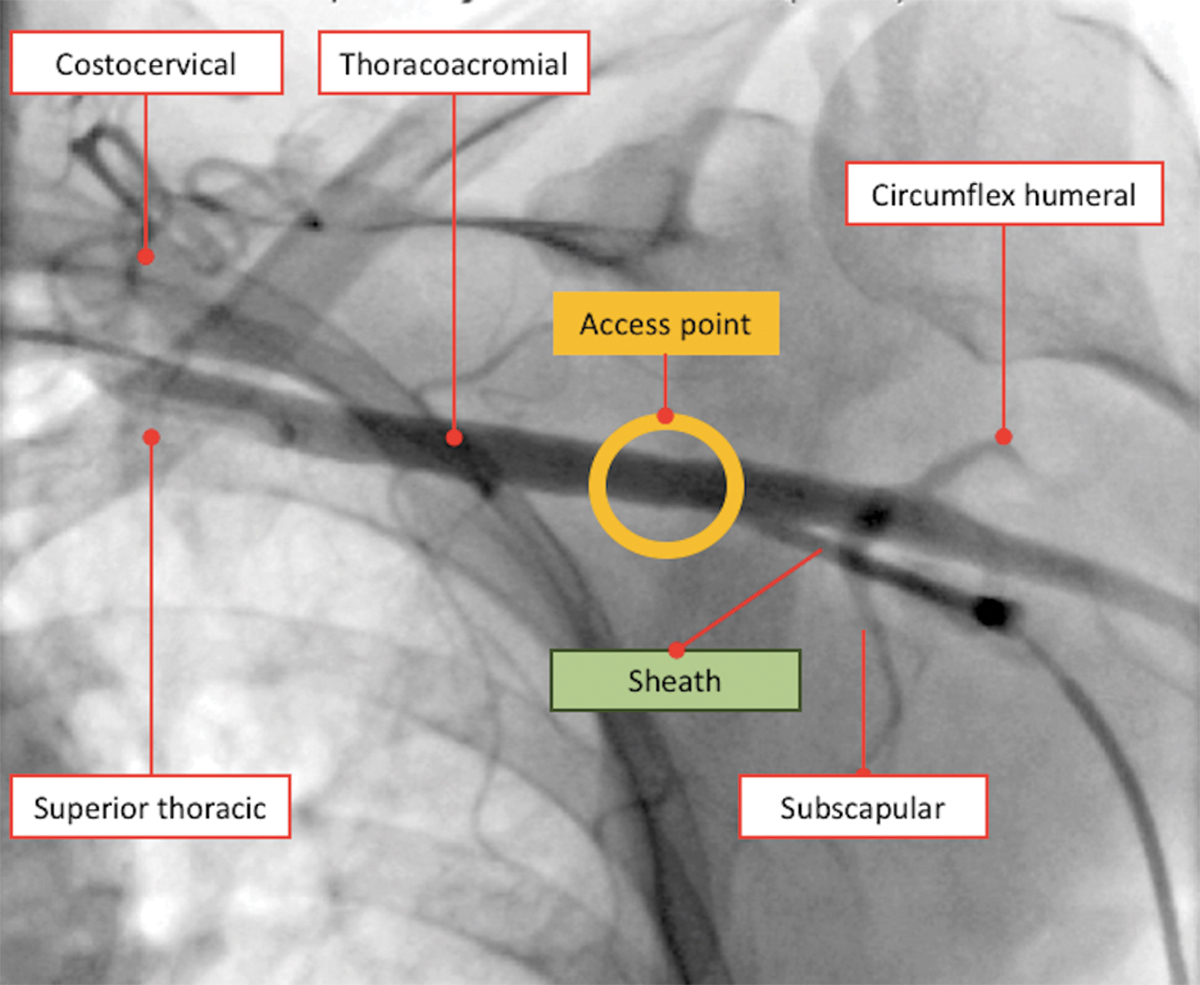
Ideally, the axillary artery should be accessed between the second and third portion at the lateral border of the pectoralis minor muscle. This is clinically important because it is associated with the lowest chance of causing brachial plexus injury, does not invade the chest and thus reduces the chance of a pneumothorax, and is manually compressible for hemostatic purposes. These landmarks are often seen using ultrasound imaging. Besides ultrasound, the practice is a selective angiogram of the subclavian and axillary arteries. Once the axillary artery and all branches are defined, the access point should be lateral to the thoracoacromial artery and medial to the circumflex humeral arteries (Figure 1).
Axillary Access for Patients Presenting with Cardiogenic Shock
For patients presenting with cardiogenic shock, unloading the ventricle is paramount to improve survival. In the case of prohibitive atheroscelorotic disease of the ilio-femoral arteries, our approach is to proceed with the axillary artery as an alternative access. Our experience has shown that by defining the anatomic and angiographic landmarks, along with the experience of performing five or more procedures, the insertion time through the axillary artery will be no longer than through femoral access, which justifies the use of the axillary access in emergent cases. “Percutaneous axillary access is a novel technique that will provide opportunities to save lives that previously were not salvageable,” says Theodore Schreiber, MD, FACC. “We believe that we are in the infancy of axillary access and that it has the potential to be a default access for large bore catheters,” he adds.
Axillary Artery Access Hemostasis
The axillary access site requires meticulous steps to guarantee safe implantation and explantation of the sheath. If there’s sufficient time, two Perclose sutures are deployed at 10 o’clock and 2 o’clock before insertion of the large bore sheath. In case of emergency when there is no time for Perclose insertion, our strategy is the following: the sheath is removed and an 8-10 mm diameter balloon (based on the vessel size) is delivered from an alternative access site (ipsilateral radial artery or femoral artery) to the arteriotomy site. Then the sheath is removed and the balloon is inflated at the arteriotomy site at 3-4 ATM (depending on the size of the vessel) until oozing stops. Sometimes a balloon inflation lasting 15-30 minutes over the arteriotomy site is needed to achieve hemostasis. If the final angiogram shows extravasation at the access site, another prolonged balloon inflation is used. If balloon and manual compression fails, then a covered stent can be used as a final bail-out strategy. In cases of a small axillary artery that is large enough to accommodate the sheath but does not allow distal flow beyond the access point, certain interventions can be done to assure sufficient perfusion to maintain limb viability. Using ultrasound guidance, a micropuncture needle is used to obtain access to the ipsilateral brachial artery. Distal to the sheath, a 5 French sheath is advanced into the brachial artery. The side arm of the sheath and 5 French sheath are then connected using a male-to-male connector creating a continuous flow from the large bore sheath to the side arm of the 5 French sheath located in the brachial artery. Flow via this bypass can also then be confirmed distally via Doppler or using standard angiography.
Axillary Access Step-By-Step
Here’s a step-by-step guide summarizing axillary access:
- Patient is prepared in the supine position with the arm abducted at 90 degrees away from the body.
- A sheath is placed in the femoral artery or ipsilateral radial artery. A JR4 catheter is advanced and used to selectively engage the left subclavian artery or innominate artery to evaluate for suitable vessel anatomy. This access also facilitates the delivery of occlusive balloons for “dry closure” of the axillary arterial access.
- Angiogram or fluoroscopic subtraction image of the subclavian and axillary arteries is performed for “roadmapping.”
- Angiographic assessment of the axillary artery and all branches is an important step to define the access point or “sweet spot” that is lateral to the thoracoacromial artery and medial to the circumflex humeral artery (Figure 1).
- After administration of local anesthesia, a micropuncture needle is advanced at a shallow angle (30-45 degrees from skin) toward the access point using fluoroscopic, angiographic or ultrasound imaging guidance.
- A 4 French microcatheter sheath is then placed and access site angiogram is performed to confirm the appropriate access point. The micropuncture sheath is exchanged for a standard 6 French sheath.
- A 0.035 inch stiff wire (e.g., Lunderquist, Amplatz Super Stiff or Supra Core) is then advanced into the subclavian artery via the 6 French sheath.
- Using a pre-close technique, two suture-mediated closure devices (Perclose ProGlide, Abbott) are deployed at the 10 o’clock and 2 o’clock positions and left uncinched.
- The arteriotomy is then sequentially dilated, prior to the introduction of the large bore sheath being used over the stiff 0.035 inch wire of choice.
- Once the procedure is completed, the device is removed from the large bore sheath.
- The subclavian or innominate artery is engaged with a JR4 catheter (or catheter of choice) from the femoral sheath. From the femoral access an exchange-length 0.035 inch wire (e.g., Glidewire Advantage) is advanced through the subclavian artery and distal to the axillary sheath into the brachial artery. However, if the ipsilateral radial artery is used, a similar exchange-length 0.035 inch wire is advanced though the subclavian artery and into the descending aorta.
- An appropriately-sized 8-10 mm x 40 mm or larger balloon (depending on vessel size) is then advanced over the 0.035 inch wire and inflated in the distal subclavian artery to occlude flow proximally. A pressure transducer can be connected to the sheath side arm to ensure that total occlusion is achieved.
- The sheath is then completely removed over the 0.035 inch wire and the pre-closure is completed by cinching and locking the previously deployed Perclose Proglide sutures.
- The balloon in the distal subclavian artery is then deflated and digital subtraction angiography is performed to evaluate for extravasation from the arteriotomy site. If no leak is noted, then the 0.035 inch wire and JR4 guide catheter are removed.
- If the final angiogram shows extravasation at the access site, another prolonged balloon inflation is used. If balloon and manual compression fails, then a covered stent (Viabahn or iCast) can be used as final bail-out strategy.
Summary
The axillary artery is considered a viable alternative access point for patients with prohibitive PAD presenting for structural heart and complex coronary interventions with fewer associated complications when compared with other alternative approaches (transcaval, transapical or transaortic).


This article was authored by Amir Kaki, MD, FACC, clinical associate professor of medicine and cath lab director; M. Chadi Alraies, MD, MPH, interventional fellow; and Theodore Schreiber, MD FACC, professor of medicine, all at Wayne State University, Detroit Medical Center, in Detroit, MI. Schreiber is also president of Detroit Heart Hospital.
References
- Mehta SR, Jolly SS, Cairns J, et al. J Am Coll Cardiol 2012;60:2490-99.
- Jolly SS, Yusuf S, Cairns J, et al. Lancet 2011;377:1409-20.
- Pedersen OM, Aslaksen A, Vik-Mo H. J Vasc Surg 1993;17:596-601.
- Pearce WH, Slaughter MS, LeMaire S, et al. Surgery 1993;114:691-7.
- Gerhard-Herman MD, Gornik HL, Barrett C, et al. J Am Coll Cardiol 2017;69:1465-1508.
- Montalescot G, Sechtem U, Achenbach S, et al. Eur Heart J 2013;34:2949-3003.
- Kurra V, Schoenhagen P, Roselli EE, et al. J Thorac Cardiovasc Surg 2009;137:1258-64.
- Judkins MP, Gander MP. Circulation 1974;49:599-602.
- Samal AK, White CJ. Catheter Cardiovasc Interv 2002;57:12-23.
- Sanghvi K, Kurian D, Coppola J. J Interv Cardiol 2008;21:385-7.
- Redfors B, Watson BM, McAndrew T, et al. JAMA Cardiol 2017;2:798-802.
- McBride LR, Miller LW, Naunheim KS, et al. Ann Thorac Surg 1989;48:874-5.
- Bruschi G, Fratto P, De Marco F, et al. J Thorac Cardiovasc Surg 2010;140:911-915.
- Tayal R, Iftikhar H, LeSar B, et al. Intl J Vasc Med 2016;2016: 3610705.
- Arnett DM, Lee JC, Harms MA, et al. Catheter Cardiovasc Interv 2018;91:150-6.
- van Mieghem NM, Lüthen C, Oei F, et al. EuroIntervention 2012;7:1340-2.
- De Robertis F, Asgar A, Davies S, et al. Eur J Cardiothorac Surg 2009;36:807-812.
- Laflamme M, Mazine A, Demers P, et al. Ann Thorac Surg 2014;97:1549-54.
- Truong HTD, Hunter G, Lotun K, et al.. Cardiovasc Revasc Med 2018;Jan 5:[Epub ahead of print].
Clinical Topics: Cardiac Surgery, Diabetes and Cardiometabolic Disease, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Prevention, Atherosclerotic Disease (CAD/PAD), Aortic Surgery, Cardiac Surgery and Heart Failure, Acute Heart Failure, Interventions and Coronary Artery Disease, Interventions and Imaging, Interventions and Vascular Medicine, Angiography, Computed Tomography, Echocardiography/Ultrasound, Nuclear Imaging, Exercise
Keywords: ACC Publications, Cardiology Interventions, Anesthesia, Local, Angiography, Angiography, Digital Subtraction, Aorta, Thoracic, Aortic Valve, Atherosclerosis, Axillary Artery, Bed Rest, Brachial Artery, Brachial Plexus, Brachiocephalic Trunk, Calcinosis, Comorbidity, Constriction, Pathologic, Coronary Artery Disease, Femoral Artery, Hemostasis, Hemostatics, Humerus, Iliac Artery, Peripheral Arterial Disease, Pneumothorax, Punctures, Radial Artery, Retrospective Studies, Risk Factors, Shock, Cardiogenic, Stents, Subclavian Artery, Supine Position, Sutures, Tomography, X-Ray Computed, Transcatheter Aortic Valve Replacement, Transducers, Pressure, Ultrasonography, Walking
< Back to Listings