Editor's Corner | DAPT, Our Genome and Clopidogrel "Resistance": Are We Near an Answer to "Which Drug, When?"
I bet few, if any, interventional cardiologists fail to prescribe dual antiplatelet therapy (DAPT) using a P2Y12 inhibitor plus aspirin after performing a PCI. After all, the ravages that balloons, stents and other devices incur on the fragile endothelial lining of arteries that result in immediate platelet deposition have been known since the early days of PCI.1
We’ve come a long way from using low molecular weight dextran, coumadin, aspirin and ticlopidine to the current DAPT combinations. But serious questions remain. Why do some patients appear “resistant” to P2Y12 inhibition with clopidogrel? (Sidestepping the aspirin resistance issue.) And if this P2Y12 resistance is real, how do we identify these patients? Does such resistance make a difference in clinical outcomes? The list of questions continues.
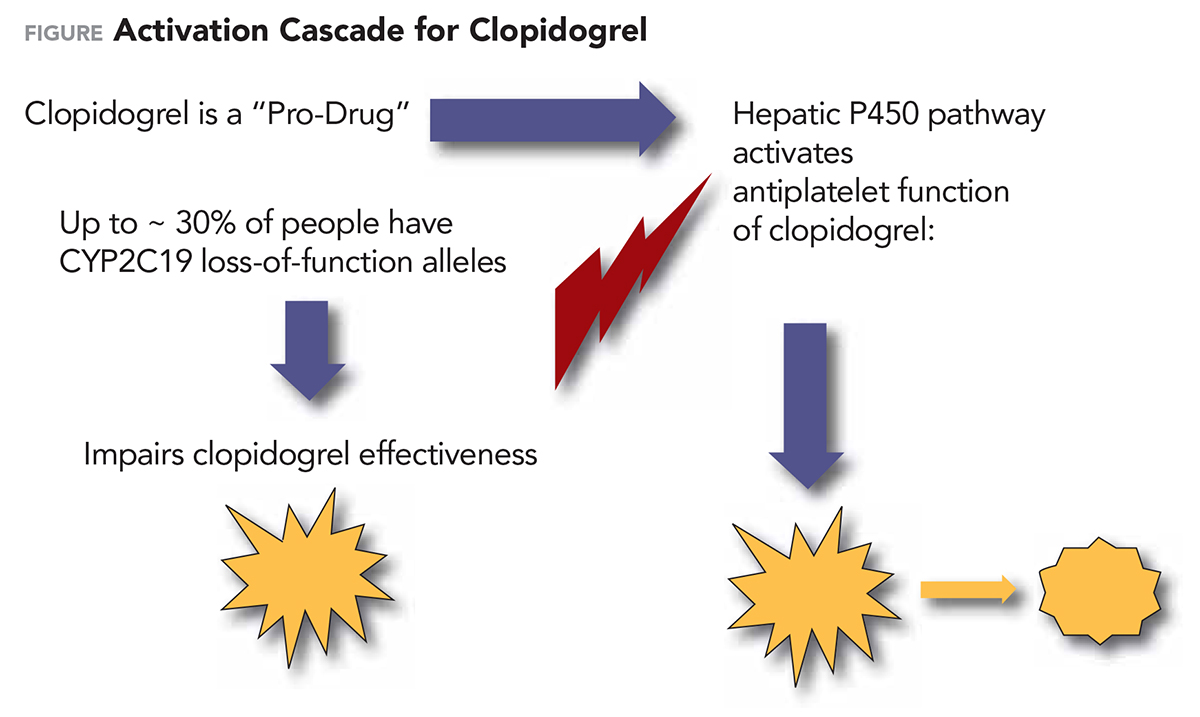
Clopidogrel “resistance” is well described. Clopidogrel is a “pro-drug.” To be effective it requires activation via the cytochrome P450 CYP2C19 pathway in the liver. But our genome may get in the way by containing within it so-called CYP2C19 loss-of-function (LOF) alleles. These alleles reduce CYP2C19 activity — resulting in reduced plasma levels of the active clopidogrel metabolite and thus less inhibition of platelet aggregation during clopidogrel therapy.
 Click image for a larger view.
Click image for a larger view.
But platelet function while on DAPT is highly variable within genetic groups — because CYP2C19 genotype and platelet reactivity are imperfect correlates of each other. Nonetheless, one might guess that patients with an LOF allele, when treated with clopidogrel after PCI, would have a higher risk of platelet-induced events. And they do! Increased major adverse cardiovascular events (MACE) have been shown in both randomized trials and patient registries comparing patients with and without CYP2C19 LOF alleles.
With all the uncertainty, or need for additional genetic testing, why not simply abandon clopidogrel and switch standard of care to alternative P2Y12 inhibitors? In fact, prasugrel and ticagrelor were better than clopidogrel in preventing MACE in acute coronary syndrome (ACS) patients in the TRITON-TIMI 38 and recent PLATO trials.2,3 The answer is that the devil is in the details.
How much better is actually better? For example, in the TRITON-TIMI 38 trial, at six to 15 months follow-up, the primary efficacy composite endpoint (cardiovascular death, nonfatal myocardial infarction [MI] or nonfatal stroke) occurred less frequently with prasugrel vs. clopidogrel (9.9 vs. 12.1 percent; hazard ratio [HR], 0.81; 95 percent confidence interval [CI], 0.73-0.90; p<0.001). The prasugrel group also beat the clopidogrel group in the rates of MI (9.7 vs. 7.4 percent; p<0.001), urgent target-vessel revascularization (3.7 vs. 2.5 percent; p<0.001) and stent thrombosis (2.4 vs. 1.1 percent; p<0.001).
All the p values make prasugrel a clear winner in TRITON-TIMI 38. But stent thrombosis (arguably the main reason a P2Y12 inhibitor is used post PCI) was only 1.3 percent less in the prasugrel group. What price was paid for that difference? Major bleeding was observed in 2.4 percent of patients receiving prasugrel and in 1.8 percent of patients receiving clopidogrel (HR, 1.32; 95 percent CI, 1.03-1.68; p=0.03). Fatal bleeding was three-times more common in the prasugrel group (0.4 vs. 0.1 percent; p=0.002).
"Platelet function while on DAPT is highly variable within genetic groups — because CYP2C19 genotype and platelet reactivity are imperfect correlates of each other."
Add to that the trial limitations. Genotype-guided therapy was not randomized and antiplatelet therapy selection was left to physician discretion in TRITON-TIMI 38. Finally, outcomes were ascertained from electronic records, without adjudication, and bleeding outcomes were not systematically collected — all worrisome limitations. The trialists themselves point out that the number of patients needed to genotype, with alternative antiplatelet therapy then prescribed for all patients with LOF alleles, to prevent one cardiovascular event was 93.
But wait — there’s more! Alternative P2Y12 inhibitors are more expensive than generic clopidogrel and their increased bleeding risk can deter its use. Safety is a problem. Even though TRITON-TIMI 38 patients were not genetically tested but simply randomized to clopidogrel or ticagrelor, the differences in efficacy outcomes across the board (though arguably small) favor prasugrel.
One option already commonly used is to simply prescribe an alternative P2Y12 inhibitor. Alternatively, should we genetically test all patients needing DAPT and use clopidogrel only in patients without LOF alleles? The problems with this strategy are that genetic testing is not always immediately available and it is expensive.
There is more information to help with this dilemma. In a secondary analysis of patients from TRITON-TIMI 38 patients with the LOF allele were estimated to have a substantial reduction in the risk of cardiovascular death, MI or stroke when treated with prasugrel compared with those treated with clopidogrel (relative risk=0.57).4 The analysis went a bit further, splitting out three groups of patients.
The overall group treated in a randomized fashion (without genetic testing) with either prasugrel or clopidogrel showed the differences in cardiovascular outcomes seen overall in TRITON-TIMI 38. Prasugrel was the winner — but not by much. The second group, testing negative for the LOF allele and able to metabolize clopidogrel to its active form, favored clopidogrel therapy for cardiovascular death and major and minor bleeding outcomes. But for the third group (those testing positive for the LOF allele) prasugrel therapy resulted in substantially less cardiovascular death and nonfatal MI — albeit at the cost of more bleeding.
One must conclude from this secondary analysis that genetic testing can indeed identify patients best treated with prasugrel or ticagrelor. Perhaps testing patients for “high on-treatment” platelet reactivity and making the appropriate switch from clopidogrel is another answer.
The one-year outcomes from PRAGUE-18 were published in January.5 It was designed to answer the question of whether prasugrel or ticagrelor therapy produced better outcomes in patients with acute MI (about 5 percent of enrollees had high-risk NSTEMI). In short, the outcomes showed no differences between the two groups. However, the actual outcome numbers were well below those in TRITON-TIMI 38, perhaps indicating a lower overall risk in the PRAGUE-18 participants or other confounding factors.
Both drugs provided good results in PRAGUE-18. Cardiovascular death, nonfatal MI or stroke at one year were 6.6 vs. 5.7 percent (p=0.50), respectively, for prasugrel vs. ticagrelor. The authors concluded that clinical use of either drug was acceptable. But then came a surprise. The study also looked at outcomes of patients who switched from their assigned study drug to clopidogrel — mostly for economic reasons. About a third of patients on prasugrel and about 45 percent of patients assigned to ticagrelor switched to clopidogrel. Patients who continued their original study medications had a higher risk of a cardiovascular event compared with the group who were economically motivated to switch to clopidogrel. Further analysis showed that the patients who switched to clopidogrel had fewer risk factors, which could well explain the differences.
But an intriguing question remains: Is there a strategy for patients such as those in PRAGUE-18 that would allow an early switch from an expensive medication (prasugrel or ticagrelor that also has greater bleeding risk) to a less expensive, lower-bleeding risk drug (clopidogrel) with associated good outcomes?
"TROPICAL ACS points out that an individualized strategy based on genetic testing and early de-escalation of antiplatelet treatment can be considered as an alternative approach in patients with ACS managed with PCI."
This strategy is supported by the recent TROPICAL ACS trial.6 This trial divided patients with ACS into standard treatment with prasugrel for 12 months (control group) or a step-down regimen (one week of prasugrel followed by one week of clopidogrel and genetic testing-guided maintenance therapy with clopidogrel or prasugrel from day 14 after hospital discharge (guided de-escalation group). Despite the medication switch, there was no increase in the combined risk of cardiovascular death, MI or stroke in the de-escalation group vs. the control group. TROPICAL ACS points out that an individualized strategy based on genetic testing and early de-escalation of antiplatelet treatment can be considered as an alternative approach in patients with ACS managed with PCI.
Thus, there is little doubt that clinical use of CYP2C19 genotyping to guide post-PCI antiplatelet strategy provides information that can result in better outcomes. How this is best used clinically remains unanswered. DAPT strategy is still based primarily on retrospective analyses and not large randomized trials. Such a randomized trial is currently underway and hopefully will be completed by 2020. TAILOR-PCI (Tailored Antiplatelet Therapy Following PCI) is designed to determine if genetic testing can identify the best antiplatelet therapy for patients undergoing PCI. Enrollees will be randomized to a conventional therapy arm (clopidogrel) without prospective genotyping guidance vs. a prospective CYP2C19 genotype-based antiplatelet therapy approach (ticagrelor 90 mg bid) in reduced-function allele patients and clopidogrel (75 mg qd) in non-LOF allele patients.
I think we can predict the outcomes of TAILOR-PCI from what we already know. Yet, having a supporting, large randomized trial will be helpful. Perhaps the investigators will also tally those patients who opt out early after initiation of DAPT using ticagrelor and switch to clopidogrel to see if the intriguing strategy of an early post-PCI switch from ticagrelor to clopidogrel suggested in the PRAGUE-18 one-year follow-up is clinically sound.
References
- Cavallari LH, Lee CR, Beitelshees AL, et al. JACC: Cardiovasc Interv 2018;11:181-91.
- Wallentin L, Becker RC, Budaj A, et al. N Engl J Med 2009;361:1045-57.
- Wiviott SD, Braunwald E, McCabe CH, et al. N Engl J Med 2007;357:2001-15.
- Sorich MJ, Vitry A, Ward MB, et al. J Thromb Haemost 2010;8:1678-84.
- Motovska Z, Hlinomaz O, Kala P, et al. J Am Coll Cardiol 2018;71:371-81.
- Sibbing D, Aradi D, Jacobshagen C, et al. Lancet 2017;390:1747-57.
Click here to read this month's Journal Wrap for more on this topic.
Clinical Topics: Acute Coronary Syndromes, Anticoagulation Management, Invasive Cardiovascular Angiography and Intervention, Anticoagulation Management and ACS, Interventions and ACS
Keywords: ACC Publications, Cardiology Interventions, Acute Coronary Syndrome, Adenosine, Alleles, Arteries, Aspirin, Blood Platelets, Confidence Intervals, Control Groups, Cytochrome P-450 Enzyme System, Dextrans, Follow-Up Studies, Genetic Testing, Genotype, Hemorrhage, Liver, Molecular Weight, Myocardial Infarction, Percutaneous Coronary Intervention, Platelet Aggregation, Platelet Function Tests, Polyethylene Glycols, Prodrugs, Prospective Studies, Registries, Research Personnel, Retrospective Studies, Risk Factors, Standard of Care, Stents, Stroke, Thrombosis, Ticlopidine, Warfarin
< Back to Listings