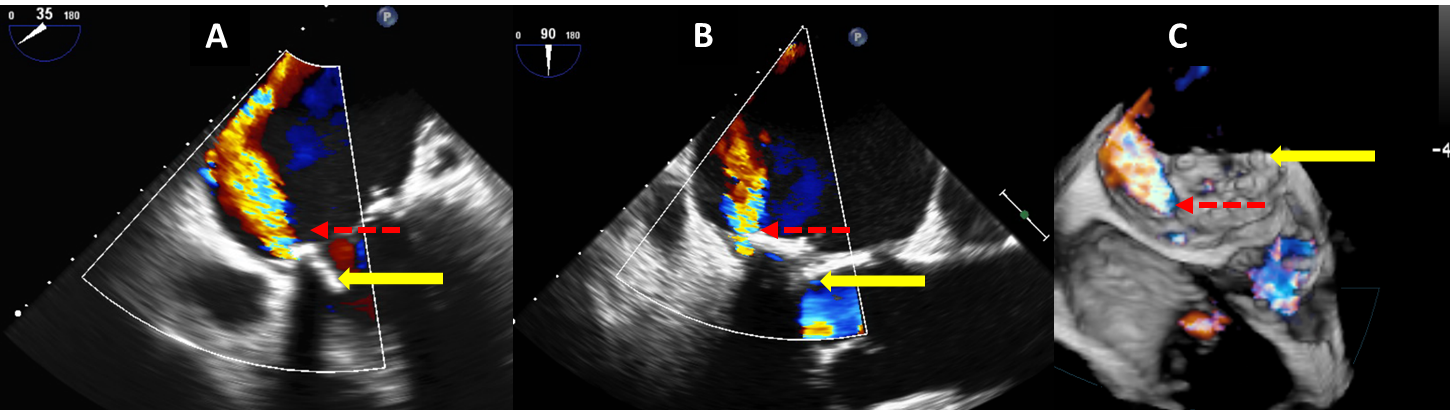
A 63-year-old man presented with increasing shortness of breath and hemolytic anemia several months after mitral valve replacement. Transthoracic echocardiogram was performed and showed a bioprosthetic mitral valve and mitral regurgitation; however this could not be well localized or quantified. Further evaluation was done using transesophageal echocardiography (TEE), which showed severe mitral paravalvular leak (PVL) (figure 1).
A, B: Two dimensional color Doppler image showing the mitral bioprosthetic valve (yellow arrow) and a turbulent jet of mitral paravalvular regurgitation (PVL, dashed red arrow). The para valvular origin of the jet is clearly depicted (see also video 1).
C: Real-time 3D color Doppler image showing the mitral bioprosthetic valve and the turbulent jet of mitral paravalvular regurgitation in similar orientation as 1B (bioprosthesis – yellow arrow, PVL – dashed red arrow) (see video 2).
What is the location of the PVL (what would you tell the surgeon/interventionalist)?
Show Answer
The correct answer is: D) At the medial aspect of the mitral valve
By convention, when referring to lesions located at or around the mitral valve, it is common practice to use the "surgical view" of the mitral valve for uniform nomenclature and proper communication.1,2,3. In this view, the mitral valve is seen "en face" from the left atrial perspective as the surgeon would view it when opening the left atrium of a patient lying in a slight left lateral decubitus position.
While looking at the mitral valve from this aspect and utilizing a "clock face" for reference, the aortic valve is seen anterior to the mitral valve at a 12 o'clock position and the left atrial appendage is seen at 9 o'clock position (figure 2A). Utilizing real time 3-dimensional (RT3D) TEE allows the operator to obtain this exact view, thus enabling accurate localization of any PVL site. While PVL sites can be seen as a defect around the mitral bioprosthetic valve (figure 2B) it is important to verify presence of flow through the defect in order to confirm that it is in fact a PVL site (figure 2C) rather than a drop out artifact. In this patient the leak is clearly seen at the 4 o'clock position. Notably, 2 dimensional TEE can also be used to localize the defect; in this patient the leak is seen medially at the 35° view (figure 1A), and postero-medially at the 90° view localizing the leak to the 3-6 o'clock quadrant. Utilizing RT3D TEE with and without color Doppler allows for even more precise localization of the leak to the 4 o'clock position (figure 1C).
Given the patient's underlying medical illnesses and the recent open heart surgery, decision was made to proceed with percutaneous repair of his PVL (figure 3). The procedure was performed under fluoroscopic and real-time 3-dimensional (RT3D) transesophageal (TEE) echocardiographic guidance.
Access to the left heart was obtained via a central venous access and a trans-septal puncture. Attempts were made to cross the PVL, however these were unsuccessful. A trans-apical puncture was then performed and the PVL was successfully crossed from this approach (figure 3A). Closure devices were advanced and positioned in the PVL site (figures 3B, C). Color Doppler interrogation showed complete resolution of the mitral regurgitation.
RT3D TEE was instrumental for guidance and proper performance of many stages of the procedure: accurate localization of the trans-septal puncture, crossing the PVL (and verifying the wire in fact crossed the PVL rather than the valve itself), visualization of the secure positioning of the closure devices, and assessing the success of the procedure and resolution of the mitral regurgitation. In addition, the echocardiographic imaging allowed for real time assessment for any possible complications that would require immediate attention and treatment (e.g. cardiac perforation, pericardial tamponade). This case highlights the importance of real time 3D echocardiographic imaging for the diagnosis of intricate cardiac pathologies, as well as for the guidance of complex percutaneous procedures for repair of structural heart diseases4.
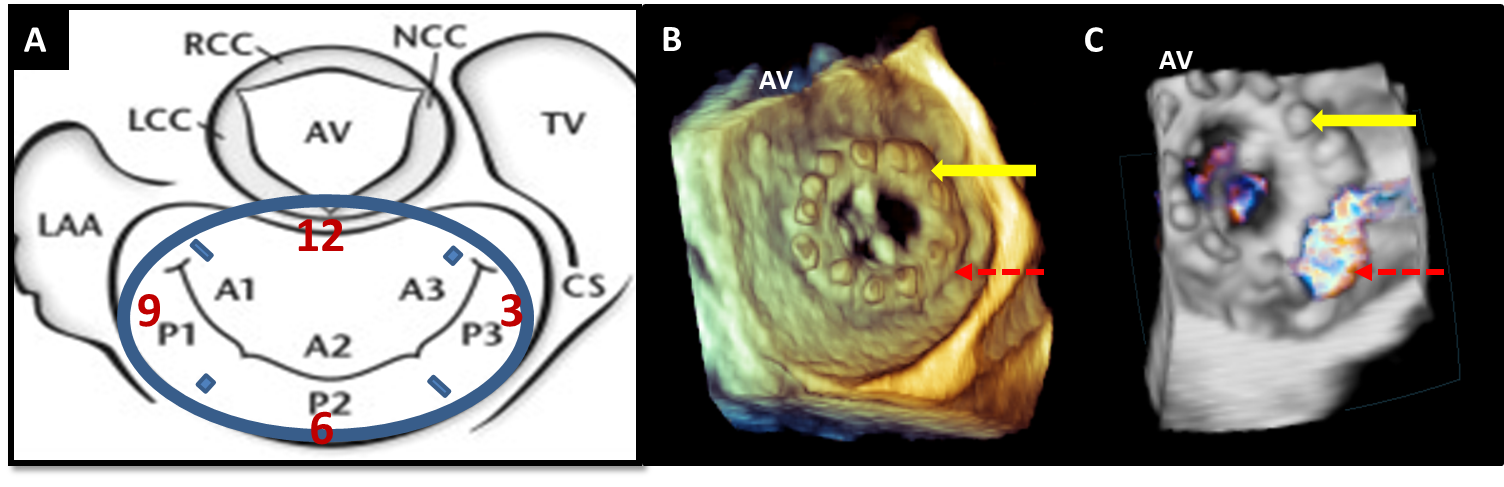
Figure 2: Localization of the PVL
A: Diagram of the mitral valve as seen from the left atrial perspective, oriented in the surgical view. In this orientation, the aortic valve is positioned at 12 o'clock, the left atrial appendage is a 9 o'clock. The interatrial septum is located at 3 o'clock, and the posterior mitral annulus is at 6 o'clock.
B: Three dimensional, en face view of the mitral bioprosthetic valve as seen from the left atrial perspective, in a "surgical view" orientation (see text). The PVL site (dashed red arrow) can be seen as a small drop out outside the mitral prosthetic ring.
C: Three dimensional color Doppler image at the same orientation clearly showing regurgitant flow across the PVL site (dashed red arrow), confirming the diagnosis of severe paravalvular mitral regurgitation originating at a 4 o'clock position (see video 3).
AV – aortic valve, LAA – left atrial appendage, TV – tricuspid valve, CS – coronary sinus, LCC – left coronary cusp, NCC – non coronary cusp, RCC – right coronary cusp.
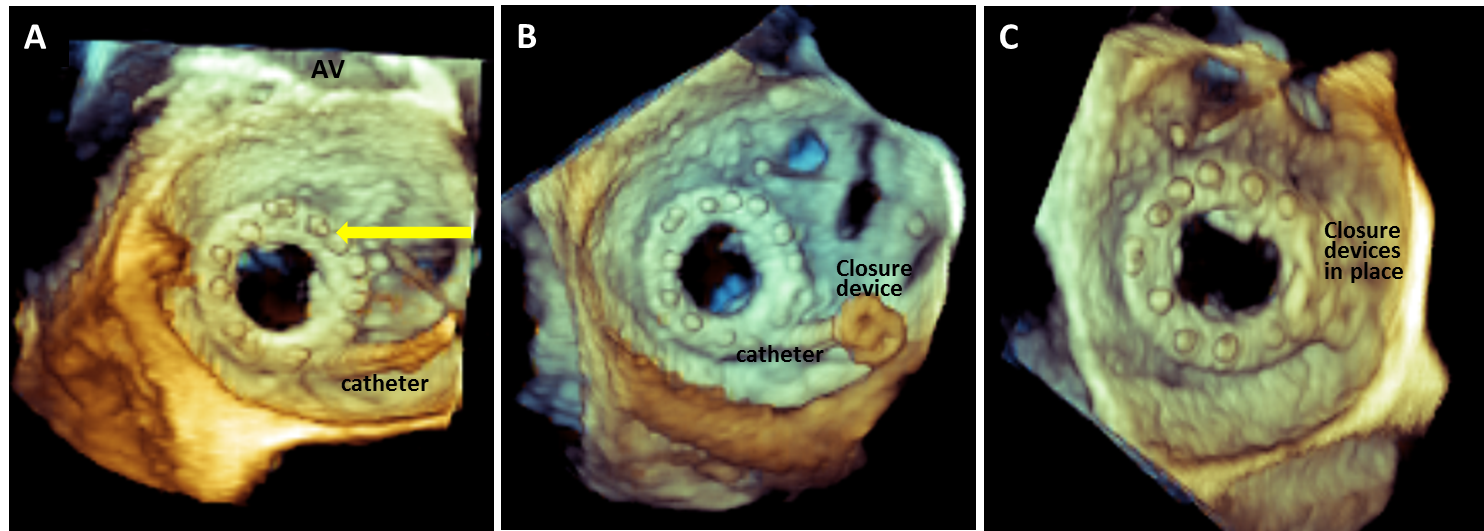
Figure 3: Percutaneous Repair of Mitral Paravalvular Leak (PVL)
Three dimensional, en face view of the mitral bioprosthetic valve as seen from the left atrial perspective, in a "surgical view" orientation.
A: A catheter is seen crossing the PVL site from the left atrium into the left ventricle (see video 4).
B: A closure device is advanced towards the PVL site (see video 5)
C: Closure devices securely in place (at the 4 o'clock position).
AV – aortic valve
Video 1
Video 2
Video 3
Video 4
Video 5
References
Perk G, Kronzon I. Interventional echocardiography in structural heart disease. Curr Cardiol Rep. 2013; 15(3): 338
Kliger C, Eiros R, Isasti G, et al. Review of surgical prosthetic paravalvular leaks: diagnosis and catheter-based closure. Eur Heart J. 2013; 34(9): 638-49
Kronzon I, Sugeng L, Perk G, et al. Real-time-3-dimensional transesophageal echocardiography in the evaluation of post-operative mitral annuloplasty ring and prosthetic valve dehiscence. J am Coll Cariolo 2009; 53(17): 1543-7
Perk G, Lang RM, Garcia-Fernandez MA, et al. Use of real time three-dimensional transesophageal echocardiography in intracardiac catheter based interventions. J Am Soc Echocardiogr. 2009; 22(8): 865-82