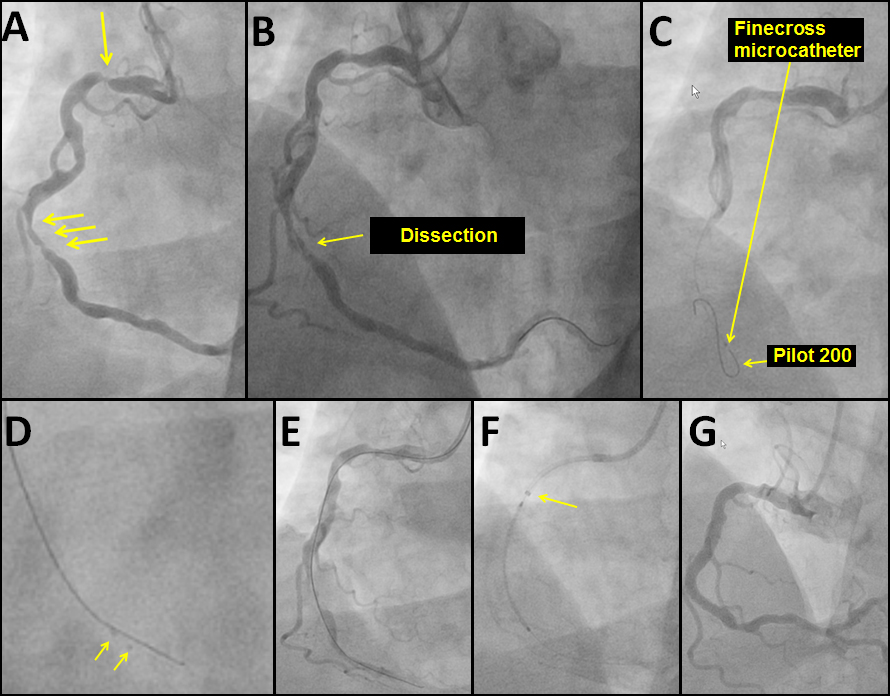
A 73-year-old man presented with a non-ST-elevation myocardial infarction. Coronary angiography revealed severe lesions in the mid and proximal right coronary artery (RCA) (Figure A). After predilation, a dissection was noted at the mid-RCA lesion (Figure B). During attempts to deliver a 3.0x38 mm stent guide and wire position was lost. Blood flow past the mid RCA lesion ceased and the patient developed chest pain and ST-segment elevations. The dissected segment could not be rewired in spite of using several guidewires (Fielder XT, Confianza Pro 12, Pilot 200, Abbott Vascular, Santa Clara California) through a Finecross catheter (Terumo, Somersit, New Jersey) or through a Venture catheter (St Jude, Minneapolis, Minnesota)
Which of following is not an appropriate treatment option at this time?
Show Answer
The correct answer is: 1. Rotational atherectomy
After coronary dissection causes acute vessel occlusion, the primary goal is to rapidly restore antegrade flow to minimize the extent of myocardial injury.
Rotational atherectomy is contraindicated in cases of dissection and moreover, there is no wire access into the distal vessel to enable advancement of the rotational atherectomy guidewire.
Emergency coronary bypass is an option, however it is not optimal in this patient with single vessel right coronary artery disease.
The Stingray balloon (Bridgepoint Medical/Boston Scientific, Natick, Massachusetts) is a 1 mm flat balloon with three exit ports connected to the same guidewire lumen.1 The distal exit port is used to place the balloon in position. The other two ports are 180 degrees opposed, so that when inflated, one is oriented to the lumen and the other toward the adventitia. Using fluoroscopy for directional orientation, the Stingray guidewire (a 0.014" high-gram guidewire with a distal tapered "probe" to grab tissue) is used to penetrate the distal true lumen and gain guidewire position.
Finally, the retrograde approach can be used to obtain access into the distal true lumen, followed by retrograde guidewire crossing, however it may require more time than antegrade dissection/re-entry.
In this patient we advanced the Pilot 200 guidewire (Abbott Vascular) to form a knucke (Figure C) which was advanced subintimally through the dissected lesion. A Stingray balloon and wire (Bridgepoint Medical, Minneapolis, Minnesota) were subsequently used to re-enter into the distal true lumen (Figure D), as confirmed angiographically (Figure E). Using a Guideliner catheter (Figure F) a 3.0x38 and 3.5x23 mm stent were delivered and successfully deployed with an excellent final angiographic result (Figure G). The patient had an uneventful recovery.
Subintimal dissection/re-entry crossing strategies are frequently used to facilitate crossing of chronic total occlusions.2,3 The present case demonstrates that the same techniques can be used to treat acute complications of percutaneous coronary interventions, such as crossing of a dissected coronary segment.4
References
Werner GS. The BridgePoint devices to facilitate recanalization of chronic total coronary occlusions through controlled subintimal reentry. Expert Rev Med Devices 2011;8:23-9.
Brilakis ES, Grantham JA, Rinfret S, et al. A Percutaneous Treatment Algorithm for Crossing Coronary Chronic Total Occlusions. J Am Coll Cardiol Intv 2012;5:367-9.
Brilakis ES, Lombardi WB, Banerjee S. Use of the Stingray guidewire and the Venture catheter for crossing flush coronary chronic total occlusions due to in-stent restenosis. Catheter Cardiovasc Interv 2010;76:391-4.
Martinez-Rumayor AA, Banerjee S, Brilakis ES. Knuckle wire and stingray balloon for recrossing a coronary dissection after loss of guidewire position. JACC Cardiovasc Interv 2012;5:e31-2.