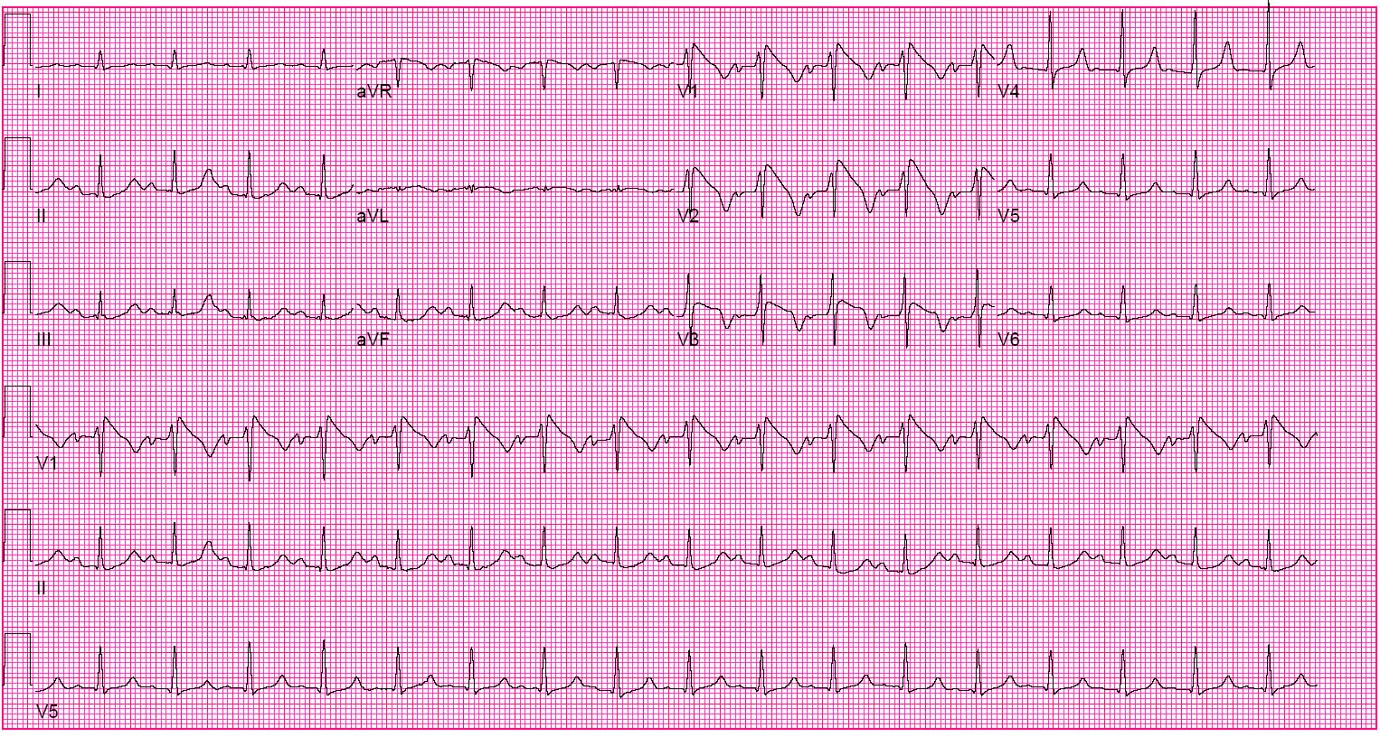
A 36-year-old male university student of far east Asian heritage with no significant past medical history presents with syncope. He is not a habitual smoker, but smokes a couple of cigarettes rarely on weekends when he watches games on TV with his friends. He has no history of hypertension, diabetes, heart failure, or renal disease. An ECG obtained at the emergency department is as shown (Figure 1), and he is referred for cardiology consultation to address the result.
Figure 1
You are asked to review the ECG and recommend next steps. Which of the following would you advise him?
Show Answer
The correct answer is: B. He has a congenital sodium channel defect and needs electrophysiology evaluation.
The ECG shows evidence of Brugada Syndrome (congenital Na channelopathy) with the classical findings of Type 1 Brugada pattern. The classic ECG signature shows ST segment elevation of at least 2 mm (0.2 mV) with a coved (downward convex) morphology, associated with an incomplete or complete right bundle branch block (RBBB) pattern followed by a descending negative T wave, with little or no isoelectric separation. It is an autosomal dominant syndrome with non-exertional syncope as hallmarks as well as far east Asian descent.
Choice A is incorrect as Brugada pattern is clearly seen. Further imaging will not contribute to the final diagnosis since these patients have a structurally normal heart.
Choice C is incorrect as the ECG changes of ST elevation are restricted to septal leads but given no reciprocal ECG changes and lack of acute coronary syndrome (ACS) symptoms, the possibility of ACS is low.
Choice D is incorrect as no delta wave is seen. QRS complex is not wide as expected in an antidromic tachycardia in WPW, where antegrade conduction occurs via the accessory pathway with retrograde conduction via the atrioventricular (AV) node.
This patient was admitted and an electrophysiologist (EP) was consulted. Since the patient presented with symptoms, an implantable cardioverter-defibrillator (ICD), was recommended. ICD is the only proven effective treatment for Brugada syndrome. There is general consensus that ICD implantation is recommended in patients with type 1 Brugada ECG (either spontaneously or after Na+ channel blockade) and a history of aborted sudden cardiac death (SCD) or related symptoms such as syncope, seizure, or nocturnal agonal respiration, given that non-cardiac causes of these symptoms have been carefully excluded.
Brugada syndrome is an inherited Sodium channel defect. Three ECG repolarization patterns in the right precordial leads are recognized. Type 1 is characterized by ST segment elevation of at least 2 mm (0.2 mV) with a coved (downward convex) morphology, associated with an incomplete or complete right bundle branch block (RBBB) pattern and followed by a descending negative T wave, with little or no isoelectric separation (our case).
The type 2 pattern has a "saddleback" appearance with a high take-off ST segment elevation of at least 2 mm, a trough displaying an ST elevation greater than or equal to 1 mm, and either a positive or biphasic T wave.
The type 3 pattern has either a saddleback or coved appearance with an ST segment elevation of less than 1 mm. These three patterns can be observed spontaneously in serial ECG tracings from the same patient or after the introduction of specific drugs.
Only the type 1 ECG pattern is diagnostic of the Brugada syndrome, with type 2 and type 3 ECG patterns being suggestive but not specific.
References
Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 2005;111:659-70 2005.
Campuzano O, Brugada R, Iglesias A. Genetics of Brugada syndrome. Curr Opin Cardiol 2010;25:210-5.
Please share your thoughts on this Patient Case Quiz in the comments section below.
Please note: You may identify yourself via the "Guest" fields, but there is no additional need to login to ACC.org in order to comment.
NEW! Improve your ECG interpretation skills with ECG Drill & Practice
This program reviews key findings in clinical electrocardiography and also contains a self-assessment ECG test, featuring the format and answer options similar to those of the ABIM’s certifying examination in cardiovascular disease. It’s a great resource for anyone preparing for initial Board certification in CV disease and for anyone looking to hone their ECG interpretation skills.