A 4-year-old male, diagnosed to have a small, pressure-restrictive, perimembranous ventricular septal defect (VSD) at 11 months of age, presents to clinic for follow-up. His mother states that he is asymptomatic but is concerned about the "loud noise that his chest made." On physical exam, both height and weight are in the 95th percentile. There is a prominent precordial impulse with a palpable thrill and a grade V/VI harsh systolic ejection murmur in the left upper sternal border with radiation to the back. There are no diastolic murmurs, clicks nor gallops. Breath sounds are clear and equal. There is no hepatosplenonomegaly, with good pulses and perfusion.
Figure 1: Electrocardiogram (ECG)
Video 1: Parasternal Short-Axis View
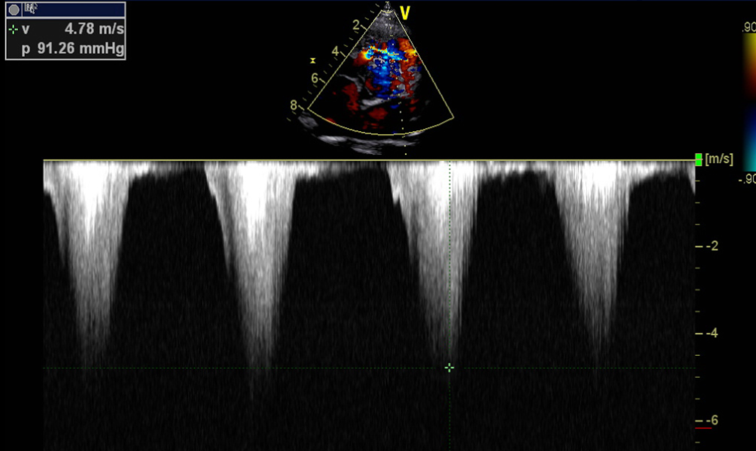
Figure 2: Doppler Still Frame Across the Right Ventricular Outflow Tract (RVOT)
Video 2: Parasternal Long-Axis View
Video 3: Apical Right Ventricular Outflow Tract (RVOT) View With Color Doppler
Video 4: Apical LVOT View With Color Doppler
Which of the following statements describes the most likely etiology of this patient's changing murmur?
Show Answer
The correct answer is: C. Double-chambered right ventricle (RV) from an RV muscle bundle.
By echocardiography, the child's VSD has spontaenously resolved. However, his physical exam is consistent with significant outflow tract obstruction – a new finding. His echocardiogram demonstrates a developing double-chambered RV (DCRV) with a prominent RV muscle bundle resulting in severe subpulmonic stenosis (Videos 1, 2, 3), with a peak velocity of 4.8 m/sec. (Figure 2). The RVOT obstruction is the etiology of the changing heart murmur. The echocardiogram also demonstrates a subaortic membrane without significant obstruction and no aortic insufficiency (Video 4). The ECG shows RV hypertrophy consistent with the echocardiogram finding of RVOT obstruction.
Acquired RVOT obstruction due to a DCRV is a known complication of VSDs.1 It is the result of hypertrophy of muscular bands within the RV that lead to a proximal high-pressure chamber and a distal low-pressure chamber with respect to the muscle bundle. The natural history is gradual worsening of the RV obstruction. The associated VSD may close spontaneously.2
Figure 2:
Doppler pattern of the RVOT shows dynamic obstruction, Vmax 4.8 ms.
The development of a subaortic membrane is also a known complication of perimembranous VSDs. As with double-chambered RV, the natural history is progressive obstruction. Aortic regurgitation is a frequent complication of a subaortic membrane, but is rarely hemodynamically significant early in the course. The regurgitation is thought to result from damage to the aortic cusps as flow passes over the subaortic membrane and becomes turbulent at the level of the valve.
For both a double-chambered RV and subaortic membrane, surgery is effective for relief of an obstruction,2 but recurrence is not uncommon.
References
Pongiglione G, Freedom RM, Cook D, Rowe RD. Mechanism of acquired right ventricular outflow tract obstruction in patients with ventricular septal defect: an angiocardiographic study. Am J Cardiol 1982;50:776-80.
Allen H, Driscoll D, Shaddy R, Feltes T. Moss and Adams' Heart Disease in Infants, Children, and Adolescents: Including the Fetus and Young Adult. 8th ed. Philadelphia: Lippincott Williams and Wilkins; 2012.