A 51-year-old woman with a history of chronic kidney disease and hypertension was brought to a community hospital with several days of intermittent chest pain and acute onset dyspnea. The initial electrocardiogram demonstrated anterior Q waves and ST segment elevation (Figure 1). Due to evolving respiratory distress and repeated episodes of non-sustained ventricular tachycardia, the patient required endotracheal intubation. Emergent angiography revealed moderate left main and severe 3-vessel coronary artery disease (CAD) with an occluded left anterior descending (LAD) artery (Figures 2-3). Due to hemodynamic instability, an intra-aortic balloon pump (IABP) was placed and, after an unsuccessful attempt at percutaneous revascularization of the LAD (felt to be chronic or sub-acutely occluded), the patient was referred to a tertiary center for further management including consideration of high risk coronary artery bypass surgery, surgical ventricular assist device implantation, and/or cardiac transplantation evaluation. Two-dimensional echocardiography prior to transfer showed an ejection fraction of 15%. She arrived to the coronary care unit on multiple inotropes and vasopressors with ongoing hemodynamic instability. She was assessed by both surgery and the advanced heart failure/transplant service. From a surgical point of view, she was deemed very high risk for surgical revascularization given her overall clinical status and questionable viability within the anterior wall. She was also deemed not an ideal transplant candidate given her current clinical status, her history of chronic kidney disease, and unclear compliance history.
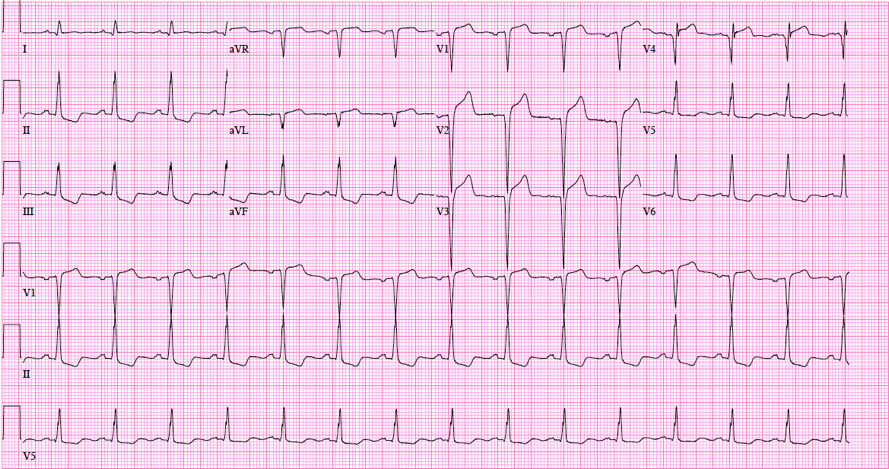
Figure 1
Presenting electrocardiogram with ST-segment elevations noted in the anterior leads and reciprocal ST-segment depressions in the inferolateral leads.
Figure 2
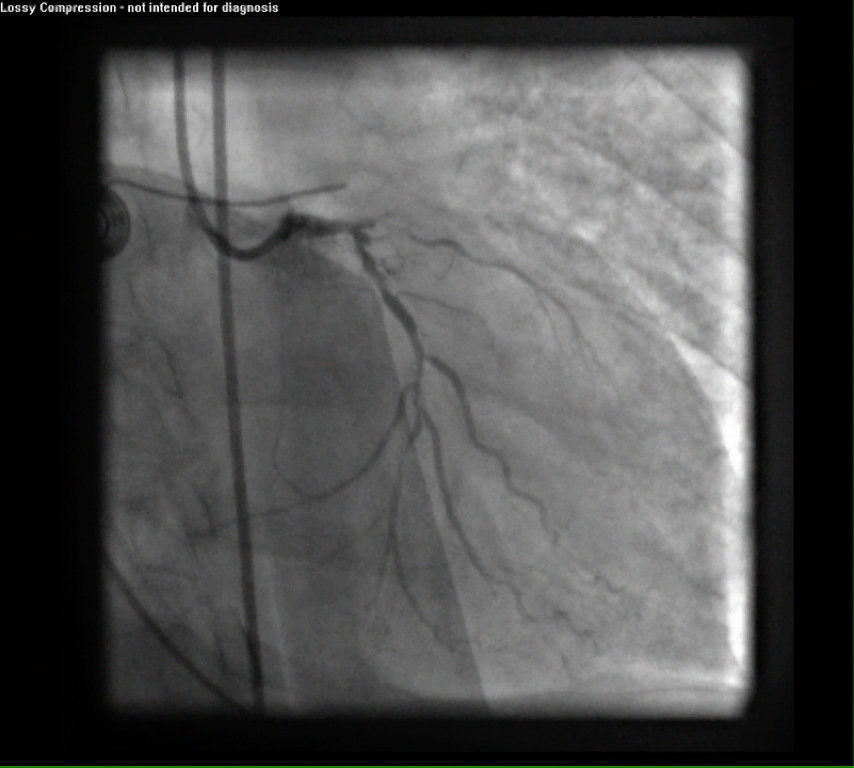
Initial left coronary angiogram in the anterior-posterior caudal projection. Notable for distal left main stenosis, LAD artery occlusion, and critical lesions in the ramus intermedius branch as well as the proximal and mid-left circumflex artery.
Figure 3
Initial right coronary angiogram in the left anterior oblique projection. Notable for significant stenosis in the proximal segment of the right coronary artery.
Which one of the following statements is correct regarding the best management option for this patient?
Show Answer
The correct answer is: B. Continue medical therapy, exchange IABP for an Impella CP® (Abiomed; Danvers, MA) left ventricular (LV) assist device, and pursue complete revascularization (CR).
This patient presented with cardiogenic shock and severe LV dysfunction due to severe 3-vessel CAD. Despite aggressive medical therapy and IABP support, the patient is still demonstrating hemodynamic instability and end organ hypoperfusion. The mortality associated with shock in the setting of ischemia is 50-60%1; this is despite significant advancements in percutaneous therapies, development of sophisticated care delivery pathways to minimize ischemic time, and advanced pharmacotherapy. Based on the results of the SHOCK (Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock) trial, early revascularization offers the most promising results in terms of improving short- and long-term mortality.2 Based on these findings, clinical practice has been to attempt to achieve CR in hemodynamically unstable patients presenting with acute myocardial infarction. Assessment of myocardial viability is not unreasonable in a hemodynamically stable patient; however, given this patient's tenuous clinical status, delaying revascularization is not likely to be of significant benefit.
The second important point to take away from this case is the importance of hemodynamic support. The 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction recommend the use of percutaneous hemodynamic support in patients with ST-elevation myocardial infarction with cardiogenic shock despite aggressive medical therapy.3,4 Moreover, the recent 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care endorses the use of percutaneous hemodynamic support during high-risk percutaneous coronary intervention (PCI), especially in those with severe LV dysfunction, as in the patient in this case.5 Although both IABP and Impella are acceptable systems of hemodynamic support, the use of more aggressive support with an Impella or tandem heart or even extra-corporeal membrane oxygenation (depending on the center's experience and the patient's clinical status) is now recommended over IABP for high-risk PCI, especially in patients with LV dysfunction. The clinical efficacy of Impella 2.5 was demonstrated in the PROTECT II (A Prospective Randomized Clinical Trial of Hemodynamic Support With Impella 2.5 vs. Intra-Aortic Balloon Pump in Patients Undergoing High-Risk PCI) study,6 and this device has been recently approved for use in patients with cardiogenic shock. The PROTECT II study randomized patients deemed inoperable with severe CAD (3 vessel CAD or left main) and severe LV dysfunction (ejection fraction < 35%) prior to PCI and followed them for up to 90 days post-PCI. The study demonstrated that the Impella was associated with improved clinical outcomes at 90 days, including improvements in major adverse cardiac and cerebral events, with the clinical benefits more prominent in those that achieved CR.7
The final important teaching point from this case is the concept of CR. Historically, surgical revascularization has aimed to achieve CR, based on early clinical data demonstrating mortality benefit in surgical patients who achieved CR compared with those who did not, especially in those with LV dysfunction.8 However, CR with PCI has only recently emerged as a goal. This is in part due to the development of drug-eluting stents, the availability of hemodynamic support, and advancements and improved success rates in recanalization of chronic total occlusions. There is now ample clinical evidence that achieving CR is clinically superior in patients with multivessel disease undergoing revascularization.9 This is also highly applicable to patients with chronic total occlusions. Emerging evidence suggests that revascularization is superior to medical therapy and that achieving CR is superior, with evidence of a mortality benefit.10,11 As such, there is now a growing movement among cardiologists and especially interventionalists to achieve CR in patients with multivessel disease who are being treated percutaneously. Thus, in our patient with 3-vessel CAD (including a possible chronic total occlusion of the LAD) and severe LV dysfunction who is deemed inoperable, the goal should be to achieve CR (including the LAD) with hemodynamic support.
This patient ultimately underwent CR percutaneously with the aid of an Impella CP LV assist device, with excellent angiographic and clinical outcome and near complete recovery of LV function on follow-up assessment 12 months post-procedure (Videos 1-3). Surgical revascularization after stabilization with hemodynamic support would have been the ideal strategy in this case, but this case does highlight that in clinical situations when surgery is of prohibitive risk, complete percutaneous revascularization with hemodynamic support is a viable option and should be pursued.
Video 1
Angiography of the left coronary system in caudal projections prior to (left panel) and after (right panel) CR.
Video 2
Angiography of the right coronary system in a left anterior oblique projection prior to (left panel) and after (right panel) revascularization of the right coronary artery.
Video 3
Echocardiography in the apical 4-chamber view prior to (left panel) and two months after (right panel) CR.
References
Westaby S, Kharbanda R, Banning AP. Cardiogenic shock in ACS. Part 1: prediction, presentation and medical therapy. Nat Rev Cardiol 2011;9:158-71.
Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med 1999;341:625-34.
Levine GN, Bates ER, Blankenship JC et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011;58:e44-122.
American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions, O'Gara PT, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61:e78-140.
Rihal CS, Naidu SS, Givertz MM, et al. 2015 SCAI/ACC/HFSA/STS Clinical Expert Consensus Statement on the Use of Percutaneous Mechanical Circulatory Support Devices in Cardiovascular Care: Endorsed by the American Heart Assocation, the Cardiological Society of India, and Sociedad Latino Americana de Cardiologia Intervencion; Affirmation of Value by the Canadian Association of Interventional Cardiology-Association Canadienne de Cardiologie d'intervention. J Am Coll Cardiol 2015;65:e7-e26.
O'Neill WW, Kleiman NS, Moses J, et al. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: the PROTECT II study. Circulation 2012;126:1717-27.
Dangas GD, Kini AS, Sharma SK, et al. Impact of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump on prognostically important clinical outcomes in patients undergoing high-risk percutaneous coronary intervention (from the PROTECT II randomized trial). Am J Cardiol 2014;113:222-8.
Bell MR, Gersh BJ, Schaff HV, et al. Effect of completeness of revascularization on long-term outcome of patients with three-vessel disease undergoing coronary artery bypass surgery. A report from the Coronary Artery Surgery Study (CASS) Registry. Circulation 1992;86:446-57.
Jang WJ, Yang JH, Choi SH, et al. Long-term survival benefit of revascularization compared with medical therapy in patients with coronary chronic total occlusion and well-developed collateral circulation. JACC Cardiovasc Interv 2015;8:271-9.
Farooq V, Serruys PW, Garcia-Garcia HM, et al. The negative impact of incomplete angiographic revascularization on clinical outcomes and its association with total occlusions: the SYNTAX (Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) trial. J Am Coll Cardiol 2013;61:282-94.
Garcia S, Sandoval Y, Roukoz H, et al. Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies. J Am Coll Cardiol 2013;62:1421-31.