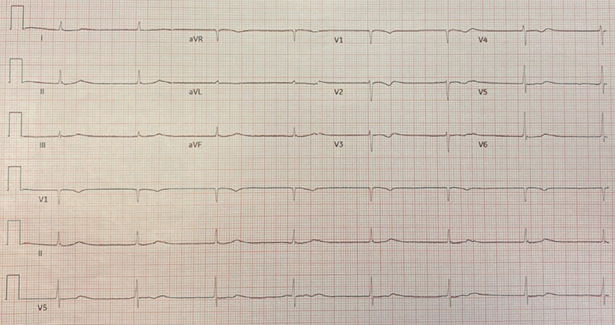
The patient is an 85-year-old female with paroxysmal atrial fibrillation (AF), hypertension, peripheral vascular disease, hyperlipidemia, and chronic obstructive pulmonary disease who presents to the clinic to follow-up on persistent AF. She is on amiodarone 200 mg PO daily, warfarin 3 mg PO daily, digoxin 125 mcg PO daily, diltiazem 300 mg PO daily, and metoprolol 25 mg PO daily. She endorses fatigue, dyspnea on exertion, dizziness, and nausea. The patient's digoxin level was 1.7 ng/mL. An electrocardiogram (ECG) (Figure 1) is performed and shows the following:
Figure 1
Figure 1
What is the most probable cause of the findings in this ECG?
Show Answer
The correct answer is: C. Digoxin Toxicity
This ECG shows a junctional escape rhythm with a heart rate of 45 beats per minute. QRS complexes are narrow with a QRS duration of 76 ms without identifiable P waves on tracing, therefore answer choice B is incorrect. There are nonspecific asymmetric T wave inversions in leads V1-V6, which do not suggest ischemia, so answer choice A is incorrect.
The correct answer is digoxin toxicity. Although this patient's digoxin level was within therapeutic limits, she was likely experiencing digoxin toxicity given her symptoms and ECG findings. Symptoms of digoxin toxicity include nausea, vomiting, abdominal pain, fatigue, weakness, visual disturbances, and cardiac dysrhythmias.1-3 Digoxin causes both increased automaticity leading to ectopy and decreased conduction through the AV node. In various studies, there are numerous ECG findings associated with digoxin toxicity including frequent premature ventricular contractions, AV block, sinus bradycardia, and AF with slow ventricular rate.1 Other dysrhythmias include paroxysmal atrial tachycardia, junctional rhythms, ventricular tachycardia, ventricular fibrillation, and biventricular tachycardia.4 A junctional escape rhythm can be caused by digoxin suppressing SA nodal impulse formation, allowing impulses from the inherent AV node, usually with rates of 40-60 beats per minute.2
ECG changes due to amiodarone include prolongation of the QT interval, widening of the QRS, sinus bradycardia, and prolongation of the PR interval.5 Of note, amiodarone inhibits the P-glycoprotein transporter, for which digoxin is a substrate, which may increase the drug serum concentration of digoxin.3 While there was no evidence of amiodarone toxicity in this patient (answer choice D), the concurrent use of amiodarone and digoxin increases the risk of digoxin toxicity. A junctional rhythm can also be seen with toxicity from non-dihydropyridine calcium channel blockers, such as verapamil and diltiazem, by slowing the recovery of both the AV and SA node.6
The patient's medications were discontinued (amiodarone, digoxin, diltiazem, and metoprolol), and her heart rate and symptoms improved. She returned to an AF rhythm, which was controlled with metoprolol only. This case highlights the importance of suspecting digoxin toxicity in a patient with non-specific symptoms and ECG changes. Furthermore, it may be beneficial to adopt a lower therapeutic range for digoxin serum concentration. Lopes et al. found that in patients with AF taking digoxin, serum digoxin level was an independent risk factor for death regardless of heart failure status, with the highest risk in patients with digoxin levels ≥1.2 ng/ml.7
References
Limon G, Ersoy G, Oray NC, Bayram B, Limon O. Retrospective evaluation of patients with elevated digoxin levels at an emergency department. Turk J Emerg Med 2016;16:17-21.
Ma G, Brady WJ, Pollack M, Chan TC. Electrocardiographic manifestations: digitalis toxicity. J Emerg Med 2001;20:145-52.
Djohan AH, Sia CH, Singh D, Lin W, Kong WKF, Poh KK. A myriad of electrocardiographic findings associated with digoxin use. Singapore Med J 2020;61:9-14.
Goldberger A. Cardiac arrhythmias due to digoxin toxicity. In: UpToDate, Post TW, ed., UpToDate, Waltham, MA. Accessed: 05/23/2022.
Giardina EG, Passman R. Amiodarone: Clinical uses. In: UpToDate, Post TW, ed. UpToDate, Waltham, MA. Accessed: 05/01/2022.
Electrocardiogram in Clinical Medicine. Lipinski MJ, Darby AE, Hudson K, Williamson K, Charlton NP, Brady WJ, Bond MC, eds. John Wiley & Sons, Ltd. 2020.
Lopes RD, Rordorf R, De Ferrari GM, et al. Digoxin and mortality in patients with atrial fibrillation. J Am Coll Cardiol 2018;71:1063-74.