This is a 41-year-old female with a past medical history of cervical cancer, s/p hysterectomy bilateral salpingectomy, s/p radiation therapy and chemotherapy, and hyperlipidemia who was transferred to our hospital for symptomatic tachycardia evaluation. She has a history of intermittent palpitations and lightheadedness.
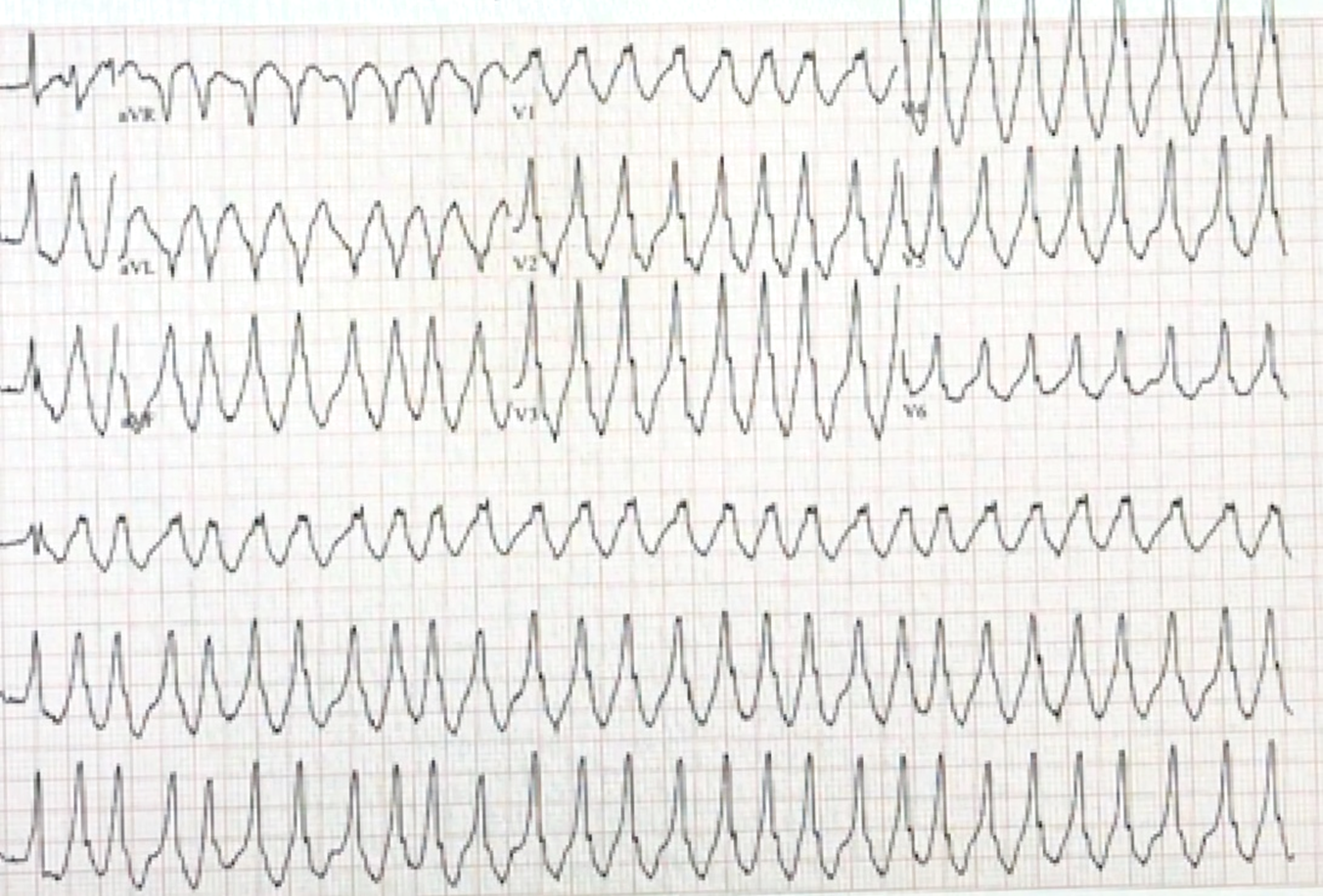
During an episode of her palpitations and lightheadedness, her cardiac monitor showed tachycardia with heart rate of approximately 200-280 beat per minute with systolic blood pressure in the 60's. The following electrocardiogram (ECG) #1 was obtained:
Figure 1: ECG #1
Figure 1
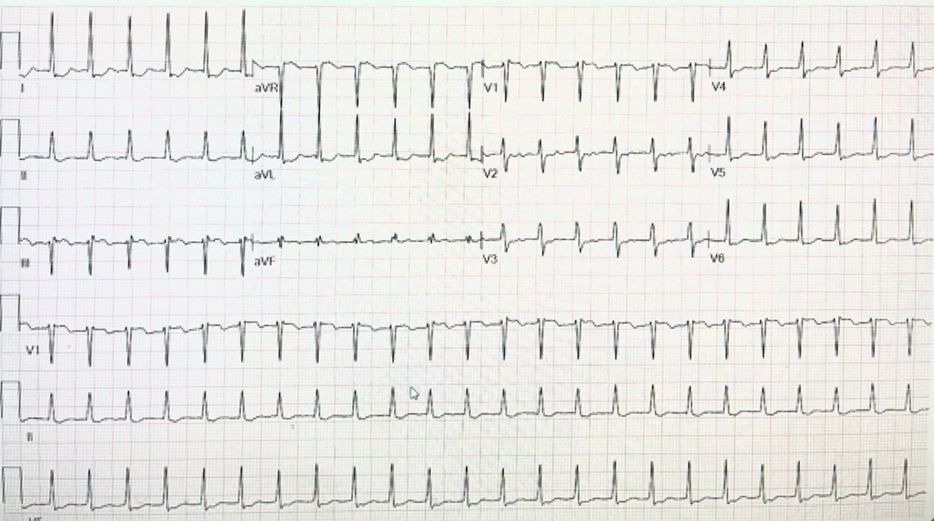
Then the rhythm changed into narrow QRS tachycardia as shown in ECG #2:
Figure 2: ECG #2
Figure 2
An intravenous push of adenosine 6 mg and 12 mg was unsuccessful necessitating direct current synchronized cardioversion with 200 joules to restore normal sinus rhythm.
She underwent an echocardiogram, which showed normal cardiac structure and left ventricular ejection fraction at 55-60%.
ECG #1 and #2 shows which of the following?
Show Answer
The correct answer is: B. Pre-excited atrial fibrillation (AF) and atrioventricular re-entrant tachycardia (AVRT)
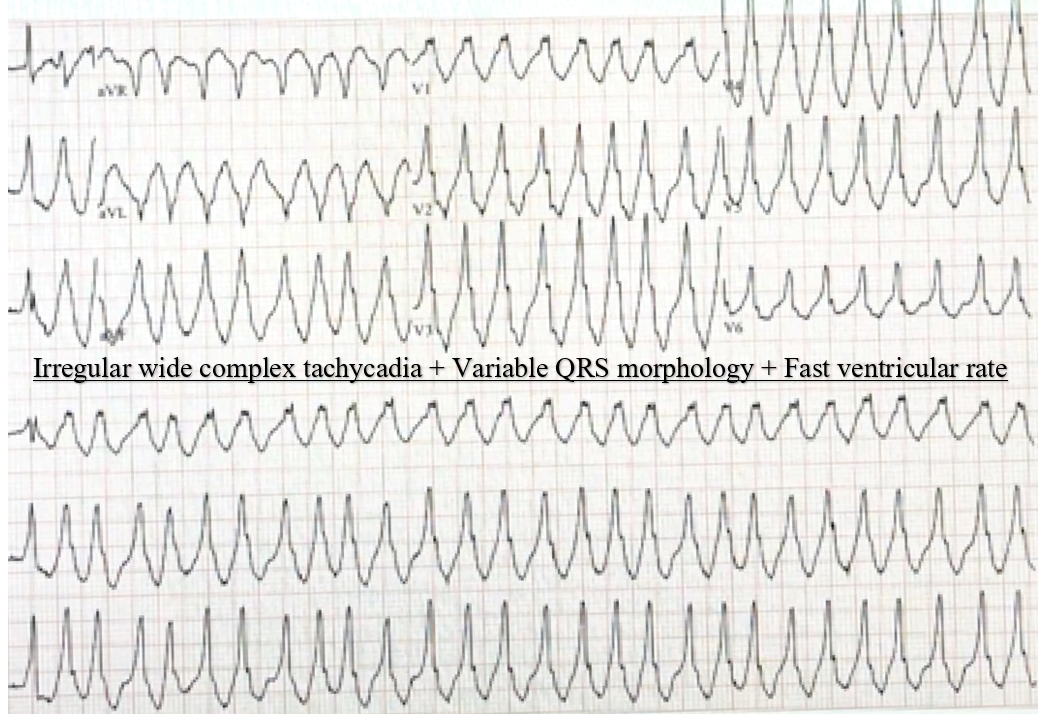
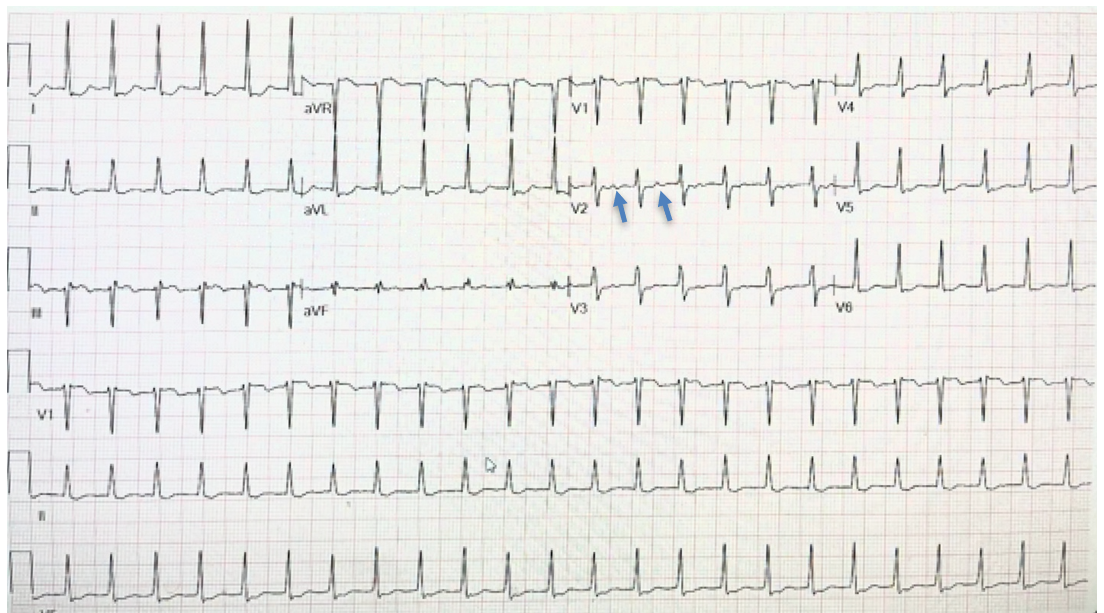
ECG #1 showed an irregular wide complex tachycardia with varying QRS morphology at a very rapid ventricular rate. These are the electrocardiographic features of pre-excited AF (AF in patients with ventricular pre-excitation). The fast heart rate (up to 280 beat per minute) is due to the short refractoriness of the accessory pathway compared to AV node. The variation of the QRS is due to variable degree of fusion from antegrade depolarization of the ventricles over the AV node and accessory pathway.1 ECG #2 showed a regular narrow QRS supraVT with RP more than 70 milliseconds (best seen in lead V2, blue arrows indicating retrograde conducted P wave), which rule out typical AVNRT. Therefore, the most likely diagnosis of the narrow QRS tachycardia is AVRT using an accessory pathway.
The patient was given intravenous (IV) push adenosine during narrow QRS tachycardia which is reasonable. However, pre-excited AF should not be treated with AV node slowing/blocking agents including adenosine, beta blockers or calcium channel blockers since slowing AV node could increase conduction over the accessory pathway, which could degenerate to ventricular fibrillation and sudden cardiac death. IV ibutilide or procainamide are the recommended drugs that usually slow the conduction over the AV node as well as accessory pathway and could terminate AF.2 However, if the patient has a fast heart rate and is unstable hemodynamically, they should be cardioverted.
The patient underwent an electrophysiological study which confirms the presence of a left sided lateral wall accessory pathway participating in antegrade conduction during AF. Assessment of the accessory pathway showed an effective refractory period (ERP) at 240 milliseconds, which is considered a high-risk pathway that could be life threatening. Pre-excited AF with very rapid ventricular response might degenerate into ventricular fibrillation and cause cardiac arrest. This patient underwent successful ablation of the accessory pathway.
Therefore, the correct answer is B: Pre-excited atrial fibrillation (AF) and AVRT.
Answer A is not correct since SVT with aberrancy should be regular.
VT could be irregular, but the degree of irregularity is significant with variable QRS duration which makes the diagnosis of VT is unlikely in a patient with normal cardiac structure and normal QT intervals. Therefore, answer C is incorrect.
Patient was symptomatic during wide complex tachycardia; therefore, answer D is incorrect.
Figure 3
Figure 3
Figure 4
Figure 4
References
Fengler BT, Brady WJ, Plautz CU. Atrial fibrillation in the Wolff-Parkinson-White syndrome: ECG recognition and treatment in the ED. Am J Emerg Med 2007;25:576-83.
January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:2246-80.