A 47-year-old highly active female with past medical history of rheumatoid arthritis (RA) presented with lightheadedness and diaphoresis after crossing the finish line at the local marathon. She was found to be in polymorphic ventricular tachycardia (VT) and was shocked three times in the field, intermittently losing consciousness but maintaining pulses. On arrival at the hospital, she was unresponsive and remained in VT for 12 minutes despite multiple defibrillations and intravenous administration of amiodarone, lidocaine, metoprolol, and magnesium. Ultimately, her rhythm degenerated into ventricular fibrillation, terminating after sedation and intubation, with brief requirement of cardiopulmonary resuscitation (CPR).
She had three prior episodes of exercise-associated syncope/presyncope (notably two were also post-marathon), with reportedly normal stress testing. Her only medication is methotrexate for RA. There was no history of smoking, excessive alcohol use, drug use, or supplement use, and she disclosed no family history of cardiovascular disease or sudden cardiac death (SCD).
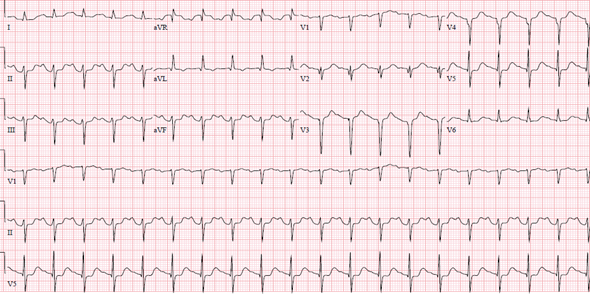
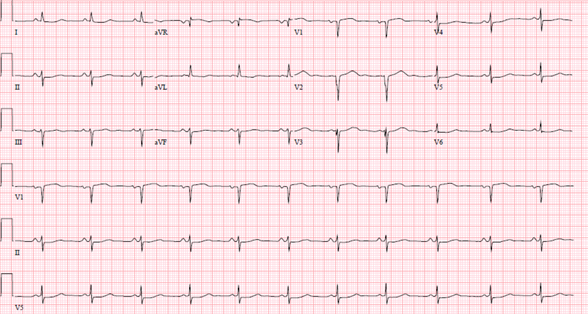
Her post-arrest 12-lead electrocardiogram (ECG) is shown in Figure 1. Echocardiogram showed a non-dilated left ventricle (LV) with an ejection fraction (LVEF) of 25%; global hypokinesis with the most significant wall motion abnormalities in the anterior, anterolateral, and apical walls; normal right ventricular size with mildly reduced function; and no significant valvular disease. Labs were notable for an initial troponin-I of 2.0 ng/ml with a peak of 26.2 ng/ml, normal electrolytes, transaminitis and transient acute kidney injury post-arrest, total cholesterol of 136 mg/dl, and low-density lipoprotein cholesterol (LDL-C) of 45 mg/dl.
Figure 1
Figure 1
Figure 1: Post-arrest 12-lead ECG showed left anterior fascicular block, septal Q waves, and a prolonged QT interval.
Figure 1: Post-arrest 12-lead ECG showed left anterior fascicular block, septal Q waves, and a prolonged QT interval.
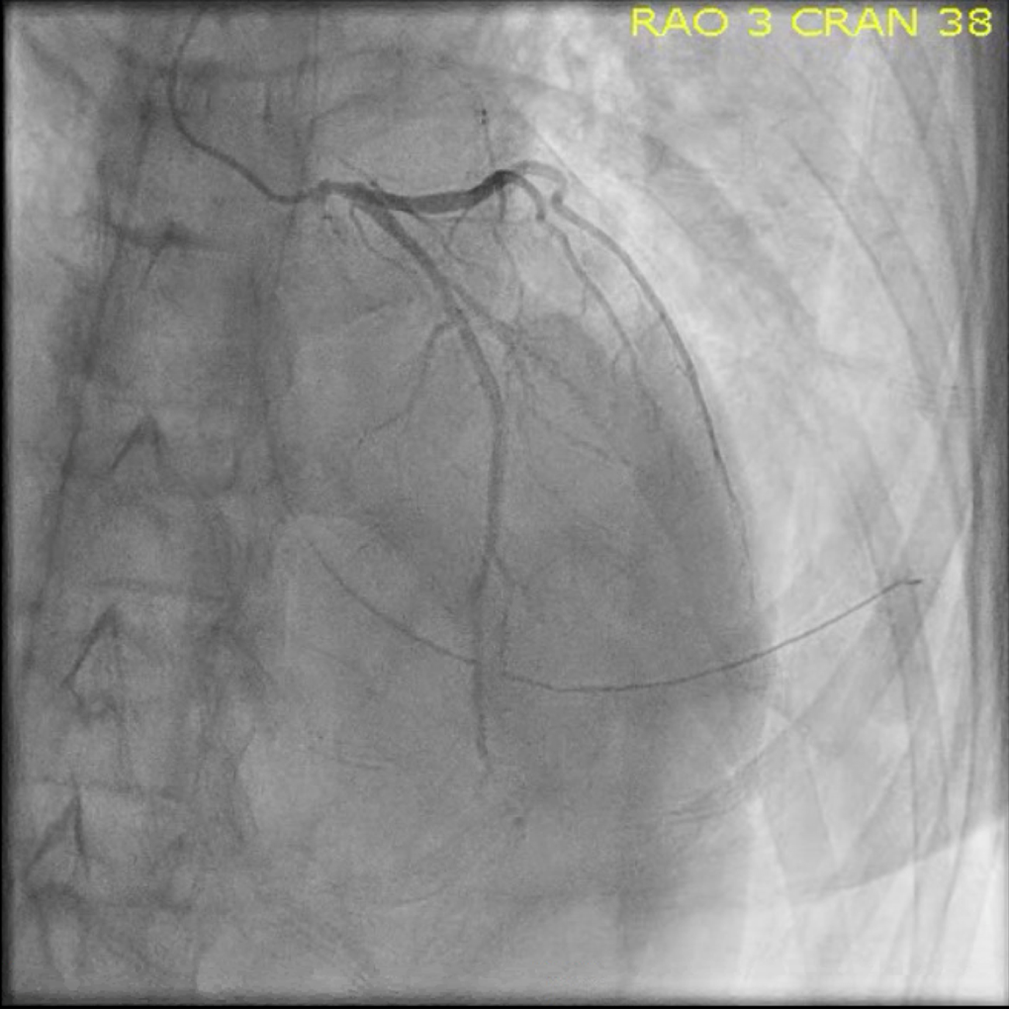
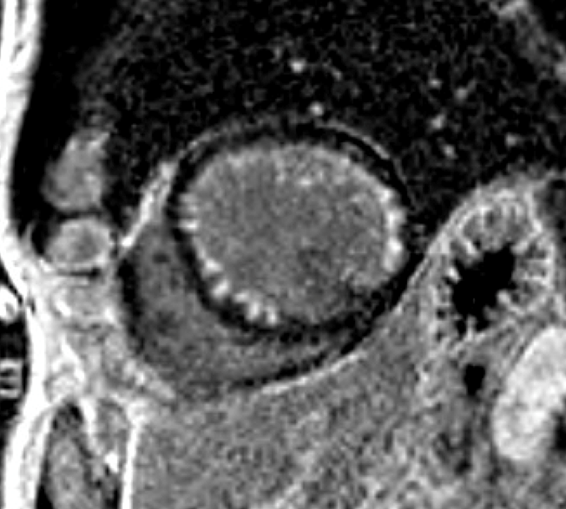
Coronary angiography was performed (Video 1 and Figure 2). There was no evidence of ruptured plaque and only mild non-obstructive atherosclerotic disease. There was dampening in the aortic pressure upon engagement of the left main artery. Cardiac magnetic resonance imaging (MRI) was subsequently performed 2 days following arrest (Figure 3). Transthoracic echocardiography performed 3 days after cardiac arrest demonstrated an LVEF of 50% with near resolution of wall motion abnormalities. ECG prior to discharge is shown in Figure 4.
Video 1
Video 1
Figure 2
Figure 2
Figure 2: Coronary angiography demonstrated mild obstructive epicardial coronary artery disease (CAD) with tapering of the distal left main artery with spasm.
Figure 2: Coronary angiography demonstrated mild obstructive epicardial coronary artery disease (CAD) with tapering of the distal left main artery with spasm.
Figure 3
Figure 3
Figure 3: Cardiac MRI showing moderate LV dilation and dysfunction, with circumferential subendocardial delayed gadolinium enhancement (LGE) of less than 50% wall thickness that spares the basal inferior and basal mid inferior segment.
Figure 3: Cardiac MRI showing moderate LV dilation and dysfunction, with circumferential subendocardial delayed gadolinium enhancement (LGE) of less than 50% wall thickness that spares the basal inferior and basal mid inferior segment.
Figure 4
Figure 4
Figure 4: ECG prior to discharge showed anteroseptal infarct, left anterior fascicular block, and normalization of the QT interval.
Figure 4: ECG prior to discharge showed anteroseptal infarct, left anterior fascicular block, and normalization of the QT interval.
What is the correct diagnosis?
Show Answer
The correct answer is: D. Coronary vasospasm
Coronary angiography (Figure 2) revealed spasm of the left main coronary artery with mild atherosclerotic disease. The cardiac MRI (Figure 3) demonstrated circumferential subendocardial late gadolinium enhancement (LGE) of less than 50% of the wall thickness that spared the basal inferior and basal mid inferior wall. The direct observation of coronary spasm and ischemic pattern of LGE on MRI in the corresponding territory with subsequent rapid recovery of LVEF led to the diagnosis and made an underlying cardiomyopathy or stress cardiomyopathy unlikely. Given that the MRI was obtained only 2 days after arrest, the subendocardial LGE may have represented scarring from repeat global ischemia induced while training.
This patient had an extensive history of high-volume, high-intensity exercise. While she had experienced prior syncopal events after prolonged endurance exercise, given the frequency with which she exercised, these events were overall rare. Coronary vasospasm is not a common diagnosis in athletes and is a rare cause of VT and SCD.1,2 Vasospastic episodes occur largely at rest, but may be triggered by exercise in some patients.2 Given the dynamic nature of coronary spasm, definitive diagnosis in autopsy studies is not possible. Hyperventilation, shifts in sympathetic/parasympathetic balance, and oxidative stress are possible reasons for our patient's recurrent episodes following prolonged intense exertion.3,4 Inflammatory disorders ̶ including RA ̶ have been implicated as risk factors for coronary vasospasm as well.5 This occurs through multiple mechanisms including endothelial damage through various inflammatory pathways, CRP-mediated activation of adhesion molecules such as ICAM-1 and VCAM-1, and reduction of nitric oxide production.5
Catheter-induced vasospasm is also a known phenomenon and was considered given the location of vasospasm in the left main artery; however, given the recurrent nature of her syncopal events and other imaging findings, exercise-related coronary vasospasm was felt to be the mechanism of her arrest.
Proposed mechanisms of coronary vasospasm include endothelial dysfunction and impaired nitric oxide release, oxidative stress, hypomagnesemia, and alterations in the Rho-kinase pathway.6 Dihydropyridine calcium channel blockers (such as amlodipine and nifedipine) have the most robust data in preventing major adverse cardiac events with coronary vasospasm and are first line therapy.7 Statins may also reduce coronary vasospasm via the Rho-kinase pathway.8 The use of beta-blockers in combined VT and vasospasm is controversial because, although beta-blockers are generally mainstays in treatment for VT, they may in fact exacerbate coronary vasospasm due to unopposed alpha-mediated vasoconstriction.9
While this patient had a very good short-term outcome, she remains at significant risk for recurrent events. In a study of 2,032 patients with vasospastic angina, patients who had survived cardiac arrest had a higher risk of cardiac death and recurrent ventricular tachyarrhythmia compared to those patients without prior cardiac arrest, which highlights the need for close follow-up and continued treatment.10 A large Japanese registry demonstrated that patients who had coronary vasospasm with an out-of-hospital cardiac arrest had a significantly lower major adverse cardiac event–free survival at 5 years (72% vs. 92% in those without cardiac arrest).2 Per the most recent American College of Cardiology (ACC)/American Heart Association (AHA)/Heart Rhythm Society (HRS) guidelines, the recommendation for ICD implantation was deemed appropriate, and due to her young age and lack of need for pacing, a subcutaneous ICD was chosen.11 She was counseled to refrain from vigorous exercise and was instructed to follow up with her cardiologist for assessment of response to treatment prior to increasing activity. She was discharged on low-dose aspirin, amiodarone, and amlodipine.
References
Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980–2006. Circulation 2009;119:1085-92.
Takagi Y, Yasuda S, Tsunoda R, et al. Clinical characteristics and long-term prognosis of vasospastic angina patients who survived out-of-hospital cardiac arrest: multicenter registry study of the Japanese Coronary Spasm Association. Circ Arrhythm Electrophysiol 2011;4:295-302.
Lanza GA, Careri G, Crea F. Mechanisms of coronary artery spasm. Circulation 2011;124:1774-82.
Boudou N, Despas F, Van Rothem J, et al. Direct evidence of sympathetic hyperactivity in patients with vasospastic angina. Am J Cardiovasc Dis 2017;7:83.
Faccini A, Kaski JC, Camici PG. Coronary microvascular dysfunction in chronic inflammatory rheumatoid diseases. Eur Heart J 2016;37:1799-1806.
Nishigaki K, Inoue Y, Yamanouchi Y, et al. Prognostic effects of calcium channel blockers in patients with vasospastic angina–a meta-analysis. Circ J 2010:74:1943-50.
Yasue H, Mizuno Y, Harada E, et al. Effects of a 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor, fluvastatin, on coronary spasm after withdrawal of calcium-channel blockers. J Am Coll Cardiol 2008;51:1742-48.
Tamura Y, Sakata K, Kawashiri M-A, Yamagishi M. Multi-vessel coronary vasospasm after beta-blocker administration. Intern Med 2018;57:3219-20.
Ahn J-M, Lee KH, Yoo S-Y, et al. Prognosis of variant angina manifesting as aborted sudden cardiac death. J Am Coll Cardiol 2016;68:137-45.
Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;51:e1-62.