

Symptomatic HCM: Diagnostic Challenge
Initial Presentation
| *Chief Complaint: | Exertional shortness of breath and chest tightness |
| History of Present Illness: | A 47-year-old woman presents with increasingly frequent and progressive shortness of breath and chest tightness with activities such as climbing one flight of stairs. She has to stop to take several breaks when using a self-propelled lawn mower on her 0.5 acre yard, which is new in the previous 1 year. She notes that she has a particularly difficult time with shortness of breath even on a leisurely walk within an hour of having eaten a meal. Once a month, she experiences episodes of palpitations and associated lightheadedness, lasting <1 min and not associated with activity. |
| Onset: | 1 year prior |
| Duration: | Symptoms persist throughout activity and resolve within 10 min of resting |
History
| Other Medical History (include comorbidities, implants, etc.): | Hypothyroidism Dyslipidemia |
| Family History: | Sister with history of tobacco abuse and myocardial infarction with stent placement at 50 years of age experienced sudden death in her sleep at 60 years of age (no autopsy performed). Another sister (60 years of age) and a brother (55 years of age) are healthy and have no medical problems. Daughter (19 years of age) and son (13 years of age) are healthy and have no medical problems. Mother is alive at 89 years of age and has atrial fibrillation. Father died at 88 years of age of multiorgan failure as a postoperative complication of coronary artery bypass graft. He had a history of myocardial infarction and congestive heart failure. |
| Social/Occupational History: | Never a smoker; drinks four glasses of wine a week; no illicit drug use history Works as a receptionist in an automotive repair shop She walks 1.6 km daily. Prior to symptom development, she had habitually run 4.8 km four times a week since her teenage years. |
Physical Findings
| *Age: | 47 years |
| *Gender: | Female |
| Race: | Caucasian |
| Height: | 1.47 m |
| Weight: | 50.3 kg |
| *Blood Pressure: | 148/83 mm Hg |
| *Pulse: | 84 bpm |
| Respiration: | 16 breaths/min |
| General Appearance: | Comfortable |
| Skin (as necessary): | No obvious lesions |
| Head and Neck: | Jugular venous pressure 6 cm H2O; normal carotid impulses |
| Chest and Lungs: | Clear lung fields |
| *Cardiac Exam: | Discrete and nondisplaced point of maximal impulse; regular rate and rhythm; grade 1/6 late-peaking systolic murmur along the left sternal border that augments to grade 2/6 with Valsalva |
| Abdomen: | Soft, nontender, nondistended, and with no organomegaly |
| Extremities (pulse, edema, etc.): | Peripheral pulses 2+ throughout; extremities warm and well perfused; no edema |
| Neurologic (as necessary): | No focal deficits and normal gait |
An electrocardiogram (ECG) is notable for sinus rhythm with left axis deviation and poor R-wave progression.
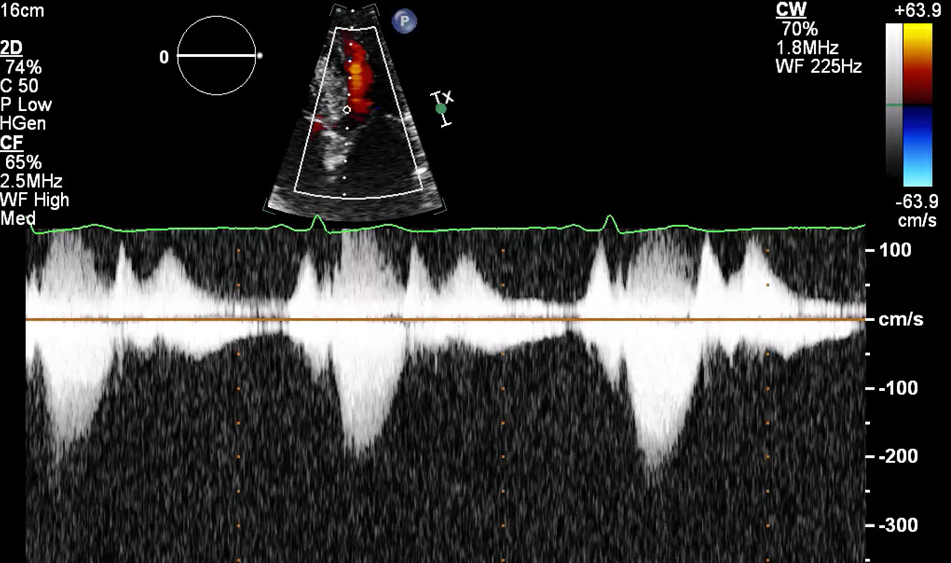
Transthoracic echocardiography reveals a small left ventricular (LV) cavity with moderate concentric LV hypertrophy and hyperdynamic LV systolic function with an ejection fraction of 75% (Figure 1). The mitral leaflets are thickened without resting leaflet systolic anterior motion. The peak pressure gradient in the LV outflow tract is 20 mm Hg (Figure 2).
Figure 1
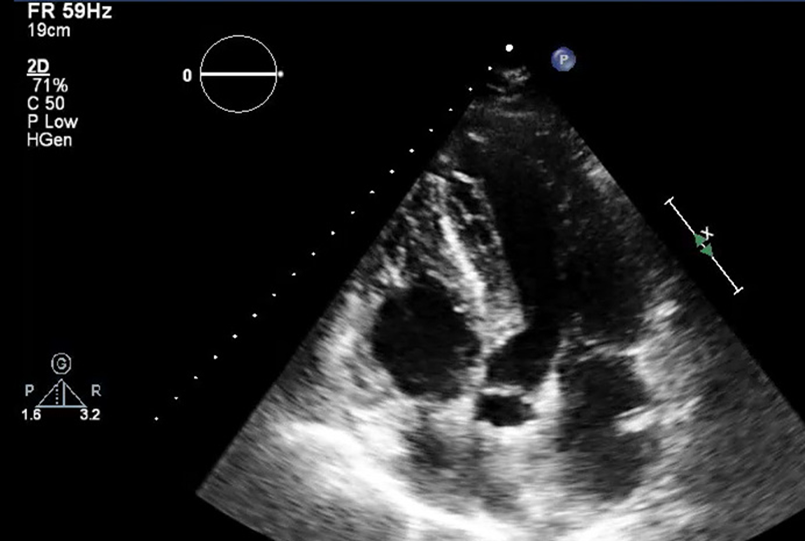
Figure 2
Which of the following tests is preferred to aid in determining the symptom etiology and management of symptoms?
Show Answer