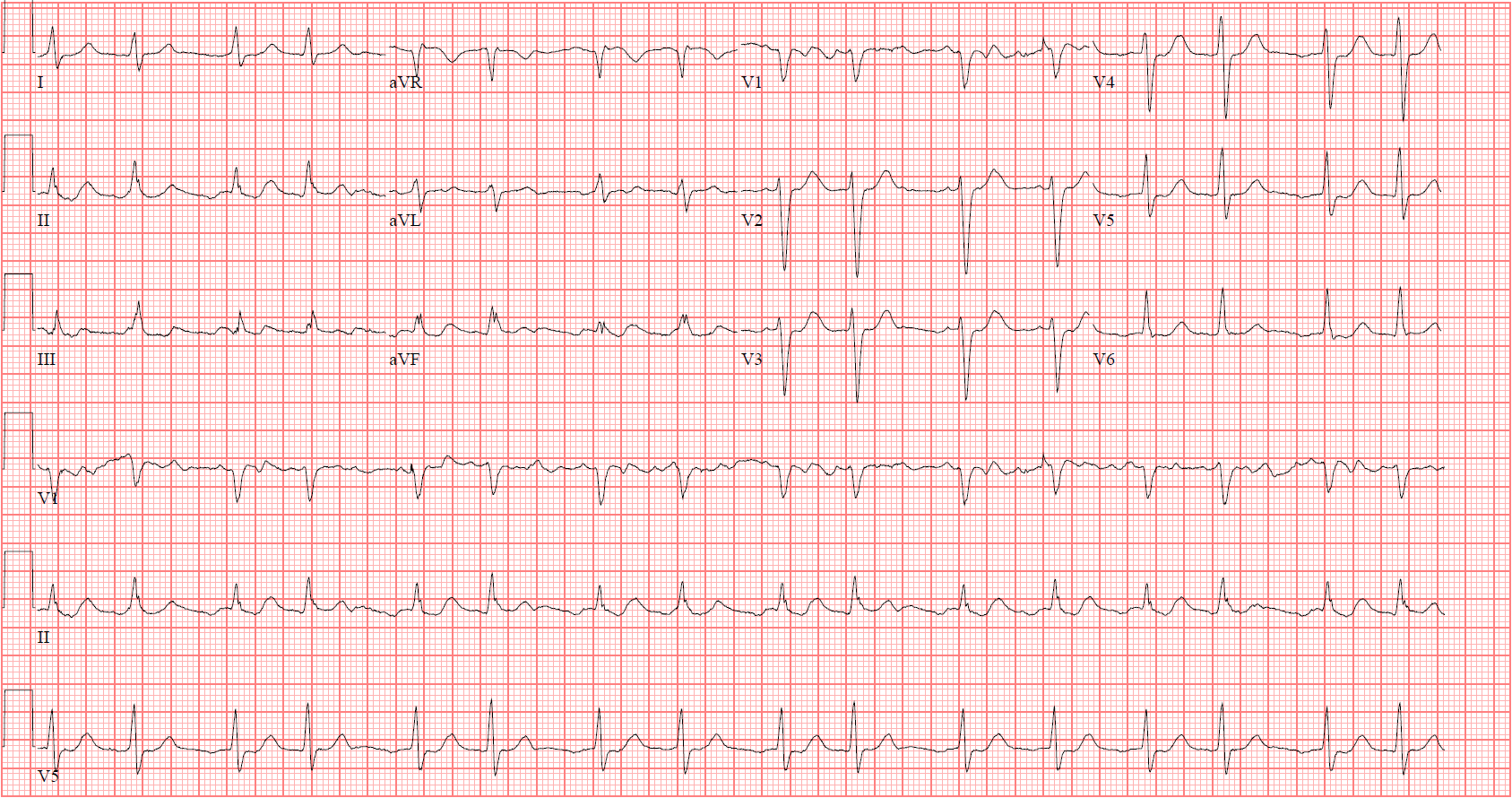
A 75-year-old male with a past medical history including type A aortic dissection with surgical repair and mechanical aortic valve replacement, paroxysmal atrial fibrillation, hypertension and hyperlipidemia presented to antiarrhythmic medications clinic for follow-up monitoring of Flecainide. The patient is asymptomatic. ECG 1 (below) is his baseline ECG.
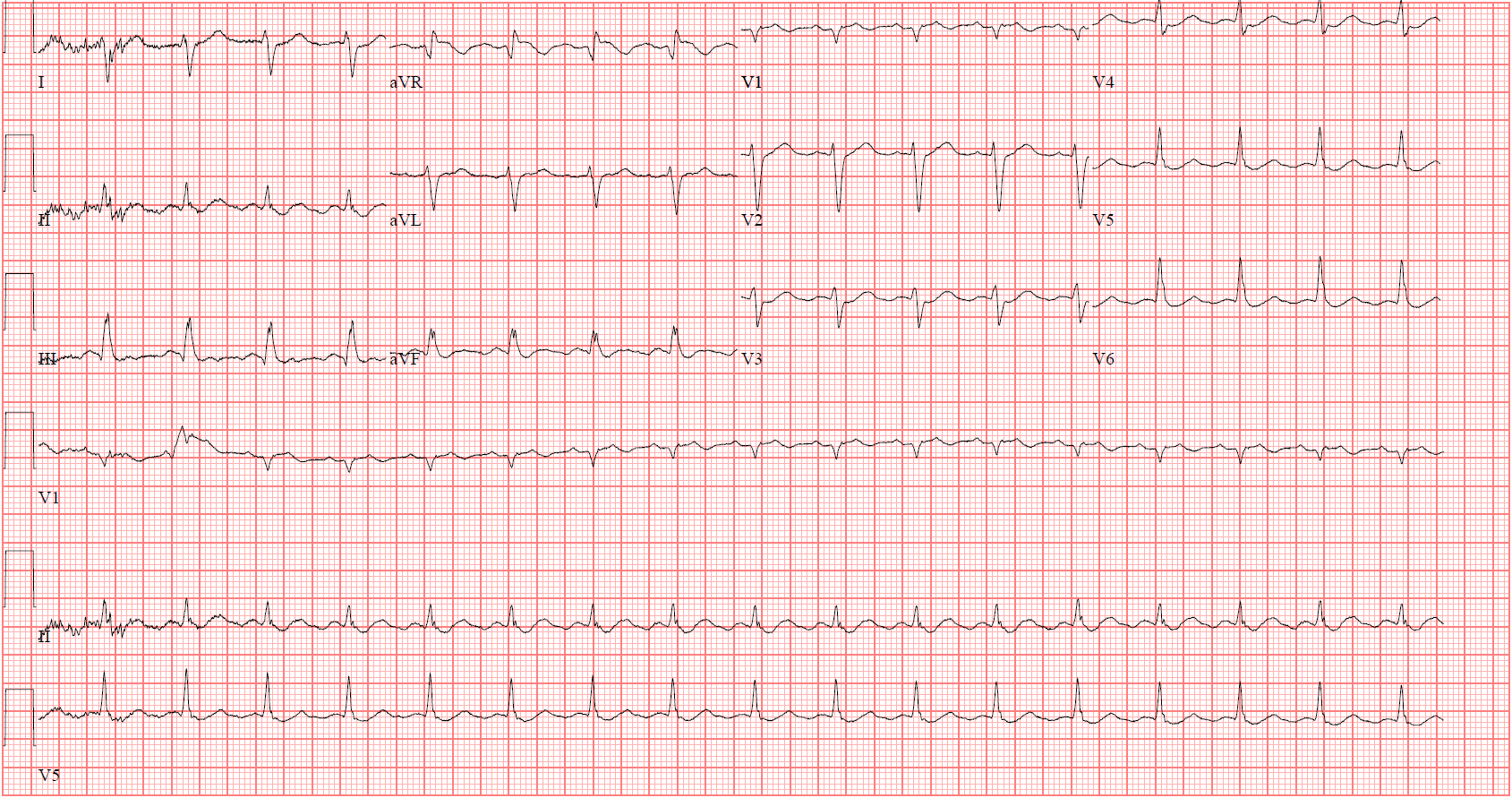
ECG 2 (below) was taken in clinic at the time of the appointment.
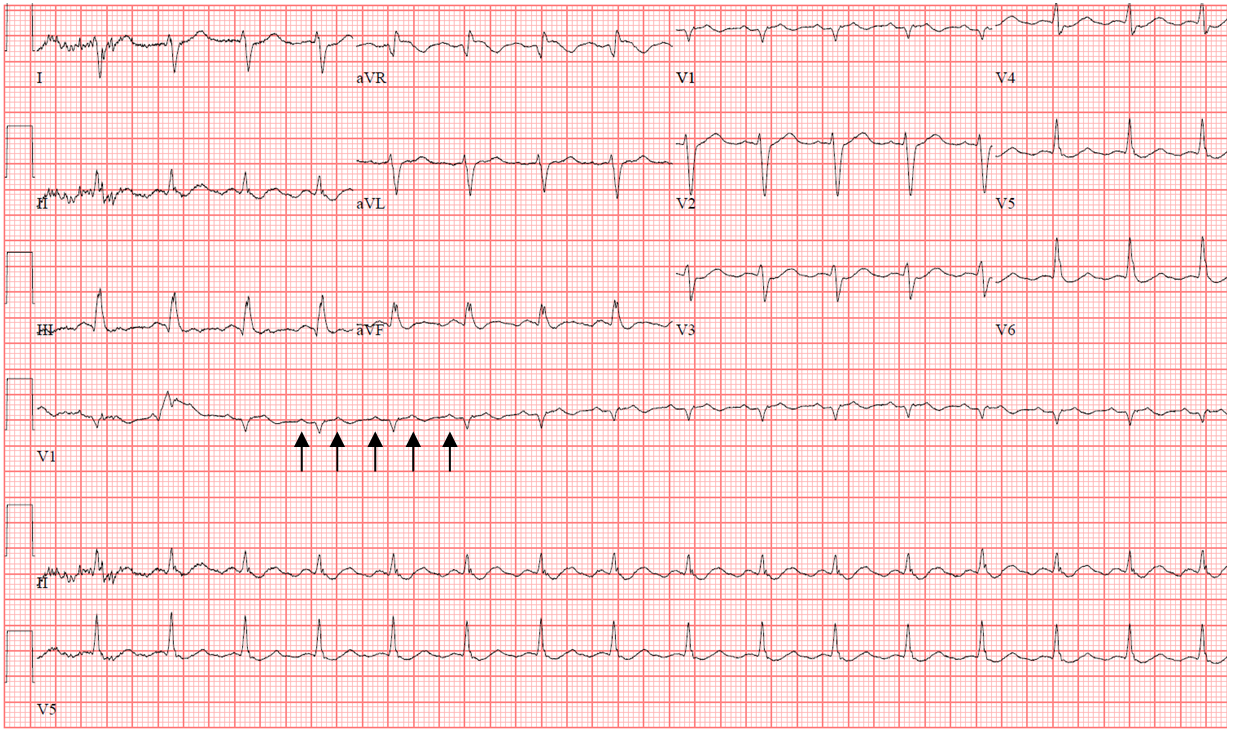
The correct answer is: C. Typical atrial flutter.
ECG 2 shows typical atrial flutter with 2:1 AV block (black arrows). Every other flutter wave is conducted through the AV node; therefore, sinus tachycardia (option A) is not correct. Accelerated junctional rhythm (option B) is incorrect because each QRS complex is the result of antegrade conduction of every other flutter wave. Finally, while this patient does have a history of atrial fibrillation, this ECG does not represent atrial fibrillation (option D). The patient is on flecainide for atrial fibrillation which caused degeneration of atrial fibrillation into atrial flutter. This is due to the pro-arrhythmic effect of flecainide, which has been reported.1
References
- Almroth H, Andersson T, Fengsrud E, et al. The safety of flecainide treatment of atrial fibrillation: long‐term incidence of sudden cardiac death and proarrhythmic events. J Intern Med 2011;27:281-90.
- Taylor R, Gandhi MM, Lloyd G. Tachycardia due to atrial flutter with rapid 1:1 conduction following treatment of atrial fibrillation with flecainide. BMJ 2010;340:b4684.