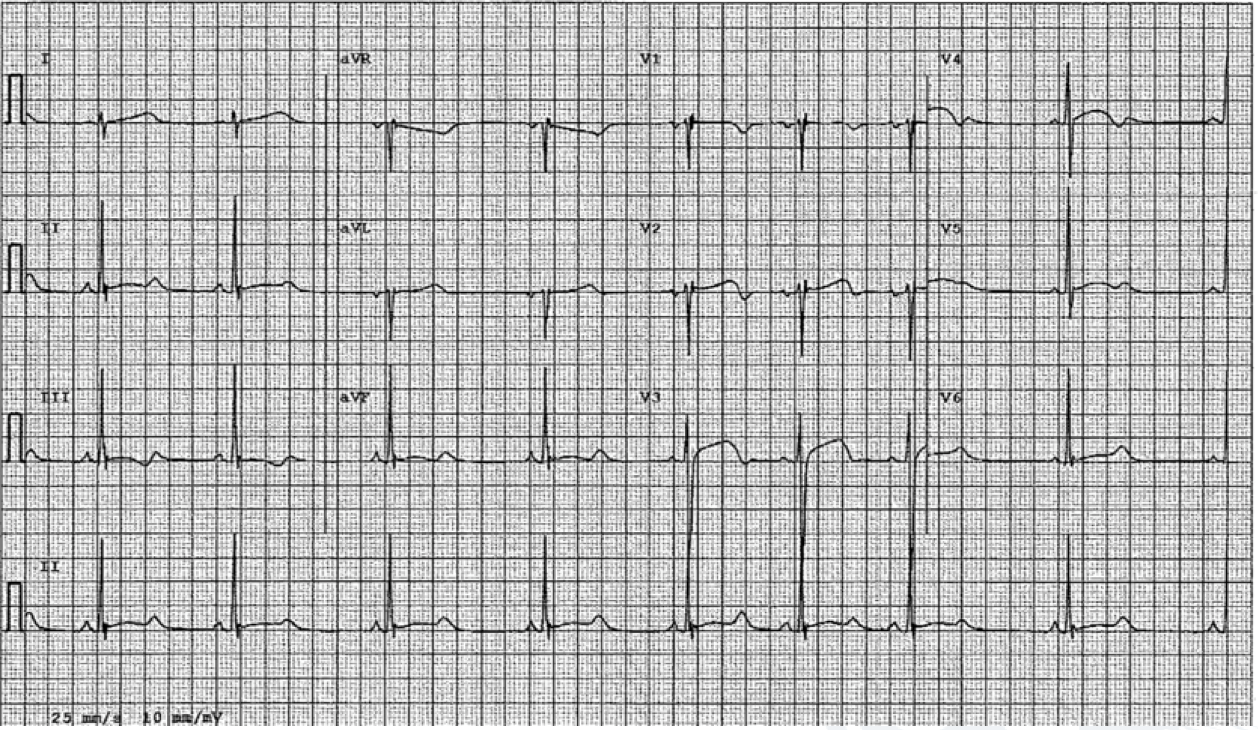
A 17-year-old male African-American American-style football player was found to have the following screening electrocardiogram (ECG, Figure 1) during pre-participation cardiovascular screening. He had no known medical history and no known family history of sudden cardiac death or inherited cardiovascular disease. He did not take any medications and denied any exertional chest pain, palpitations, shortness of breath, lightheadedness, seizures or syncope. The physical examination was unremarkable. With this ECG, he proceeded with an exercise treadmill test, which did not elicit any ventricular arrhythmias, but the QTc interval persisted at 556ms 2 minutes into the recovery period. Further genetic testing revealed a mutation in the KCNH2 gene affirming the diagnosis of congenital Long QT Type 2.
Figure 1
Figure 1
What is the next best step in management?
Show Answer
The correct answer is: D. Start nadolol
This is a case description of an asymptomatic competitive football player with congenital Long QT2 syndrome.
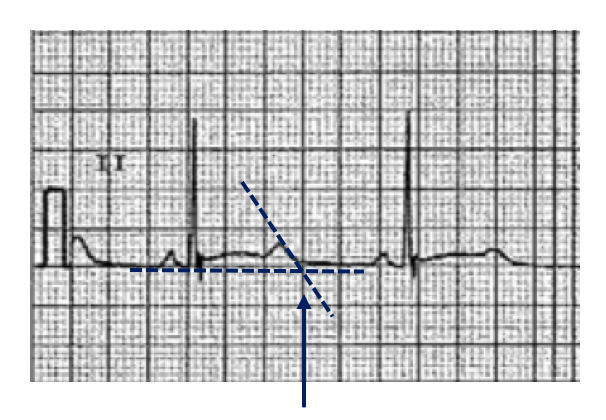
The QTc in the screening ECG (Figure 1) was calculated at 544ms using the Bazett's heart rate correction formula [QTc = QT / √RR (sec)].1 The 'teach the tangent' approach was used to delineate the end of the T wave.2 A tangent was drawn to the steepest slope of the last limb of the T wave in lead II (or lead V5 (Figure 2)) and the end of the QT interval was measured at the intersection of the tangent with the baseline.2 It is important to note that the Bazett's formula loses accuracy at heart rates <50 or >90 bpm and should be considered when applying this methodology in the estimation of the corrected QT interval.3
Figure 2
Figure 2
Based on the 2015 eligibility and disqualification recommendations for competitive athletes with cardiac channelopathies, competitive sports participation may be considered in males with QTc >470ms, with the exception of swimming in a previously symptomatic Long QT1 patient, provided treatment and appropriate precautionary measures are instituted and the athlete has been asymptomatic on treatment for at least 3 months.4 Beta blocker therapy is considered the mainstay treatment for Long QT syndrome and resting QTc >470ms.5 Regarding the choice of beta blockers, expert consensus favors the use of nadolol (choice D), a non-cardioselective beta-blocker, rather than cardio selective beta-blockers such as metoprolol (choice B).6 Left cardiac sympathetic denervation (choice E) or implantable cardioverter defibrillator (ICD, choice A) are options for treating symptomatic Long QT in high risk patients in which beta blocker therapy is ineffective or not well tolerated and intensification of therapy is warranted.5
This case also incorporates the concept of shared decision-making regarding sports eligibility in athletes with cardiovascular disease. The shared decision-making model involves the athlete, athlete's family, school and team officials, and other pertinent stakeholders in the decision making process regarding return to play, following the implementation of appropriate risk stratification and individualized treatment with a clear understanding of the potential risks.
Specific to Long QT, in a registry of 130 competitive athletes with long QT syndrome who remained in competitive athletics, there were two cardiac events reported (no deaths) during a mean follow-up period of 5.1 ± 2.9 years.7 The cardiac events were ICD shocks for ventricular fibrillation in an athlete who was non-compliant with beta blocker treatment.7 A second study reported no sports related cardiac events or deaths (mean follow up period of 7.1 ± 4 years) in a registry of 103 Long QT syndrome patients who continued to participate in sports.8
Observations from these studies have been referenced in the most recent sports eligibility guidelines regarding Long QT syndrome and sport participation.4 However, we caution generalizing these data to all athletes with Long QT syndrome. It remains prudent to approach each athlete with Long QT syndrome in an individualized manner, recognizing the limitations in the current data available and appreciating the sport-specific and inherent risks that may or may not be present in the athlete.
In the case presented, the athlete tolerated once daily dosing of nadolol 80mg with normalization of the QTc interval. The patient, his family, and his athletic team were counselled on the avoidance of QT prolonging drugs and to institute a careful emergency action plan. After 3 months of sustained nadolol therapy, repeat normal Holter monitoring, and normal exercise testing, the athlete, athlete's family, and university agreed upon a return to competitive football after extensive and repeated shared decision-making meetings with the healthcare team.
References
Bazett HC. An analysis of the time-relations of electrocardiograms. Heart 1920;353–370.
Postema PG, De Jong JS, Van der Bilt IA, Wilde AA. Accurate electrocardiographic assessment of the QT interval: teach the tangent. Heart Rhythm 2008;5:1015-8.
Sharma S, Drezner JA, Baggish A, et al. International recommendations for electrocardiographic interpretation in athletes. Eur Heart J 2018;39:1466-80.
Ackerman MJ, Zipes DP, Kovacs RJ, et al. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 10: the cardiac channelopathies: a scientific statement from the American Heart Association and the American College of Cardiology. J Am Coll Cardiol 2015;66:2424-8.
Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 2018;15:e190-e252.
Ackerman MJ, Priori SG, Dubin AM, et al. Beta-blocker therapy for long QT syndrome and catecholaminergic polymorphic ventricular tachycardia: are all beta-blockers equivalent? Heart Rhythm 2017;14:e41-e44.
Johnson JN, Ackerman MJ. Return to play? Athletes with congenital long QT syndrome. Br J Sports Med 2013;47:28–33.
Aziz PF, Sweeten T, Vogel RL, et al. Sports participation in genotype positive children with long QT syndrome. J Am Coll Cardiol EP 2015;1:62-70.