An 83-year-old male patient who was an ex-smoker with a medical history of diabetes mellitus, hypertension, and stage 3 chronic renal impairment presented with intermittent, variable threshold exertional angina for a few weeks. His symptoms persisted despite optimal medical treatment. His vital signs were stable, and his physical exam was unremarkable. An electrocardiogram showed sinus rhythm with T inversions over the anterior leads. An echocardiogram revealed left ventricular ejection fraction of 45-50% with severe hypokinesia over anterior wall.
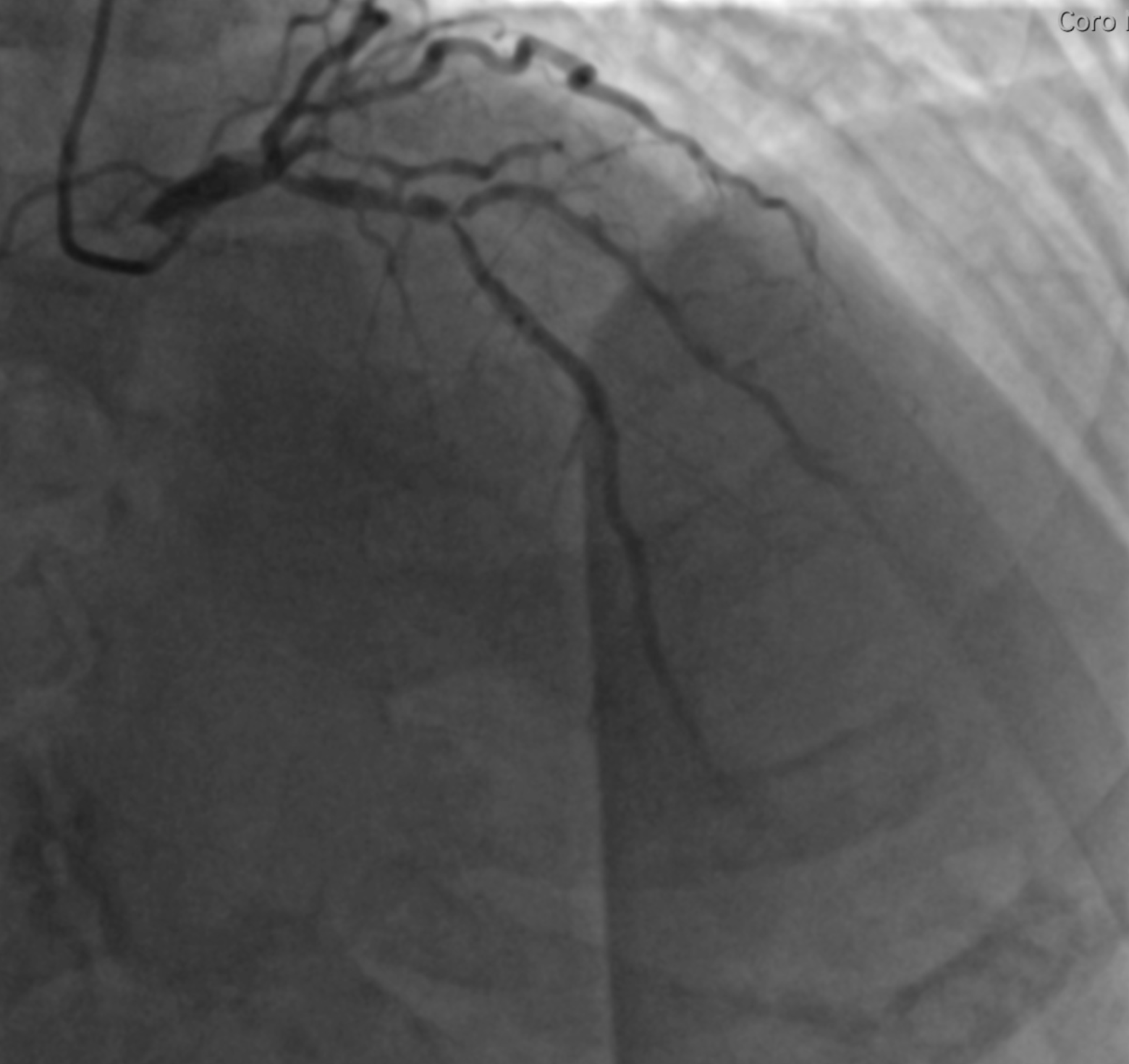
His coronary angiogram showed moderate ~40-50% stenosis from distal left main artery (LM) to ostial left anterior descending artery (LAD) (Medina 1,1,0) and critical ~99% stenosis over proximal LAD-diagonal bifurcation (Medina 1,1,1) (Figures 1-2). Fractional flow reserve (FFR) was performed with pressure wire at proximal left circumflex artery (LCx), which showed minimal value 0.83 at maximal hyperemia. Calculated Society of Thoracic Surgery score of this gentleman for coronary artery bypass grafting surgery (CABG) was 4.59%. SYNTAX score for LAD-diagonal percutaneous coronary intervention (PCI) was 11, and SYNTAX score for LM and LAD-diagonal PCI was 24.
Figure 1
Figure 1
Figure 2
Figure 2
What is the most appropriate next step in this patient's management?
Show Answer
The correct answer is: E. Perform intravascular ultrasound (IVUS) of LM lesion
The patient presented with exertional angina despite optimal medical treatment, so answer A is not correct. An echocardiogram already showed impaired left ventricular systolic function with regional wall hypokinesia compatible with the finding of critical LAD stenosis in coronary angiogram.
Answers B, C, or D could be the final management of this gentleman, but it depends on the severity of the distal LM lesion. Although FFR was negative (minimal value 0.83) with the pressure wire placed in the non-diseased LCx, the actual blood flow across the LM lesion was affected by the flow across both downstream vessels (i.e., both LAD and LCx). The presence of significant stenosis over downstream LAD may decrease the flow and hyperemic gradient across LM, resulting in falsely elevated FFR number with pressure wire placed in non-diseased LCx.
Fearon et al.1 showed that for patients who have severe stenosis in one major branch of the LM, if FFR of the LM is either >0.85 or ≤0.80, then the LM lesion can be treated as hemodynamically insignificant or significant, respectively. If FFR is between 0.80 and 0.85, then the hemodynamic significance of LM lesion cannot be accurately determined if combined FFR of the LM and downstream lesion is ≤0.45.2 Additional assessment such as IVUS is preferred to determine severity of LM lesion.
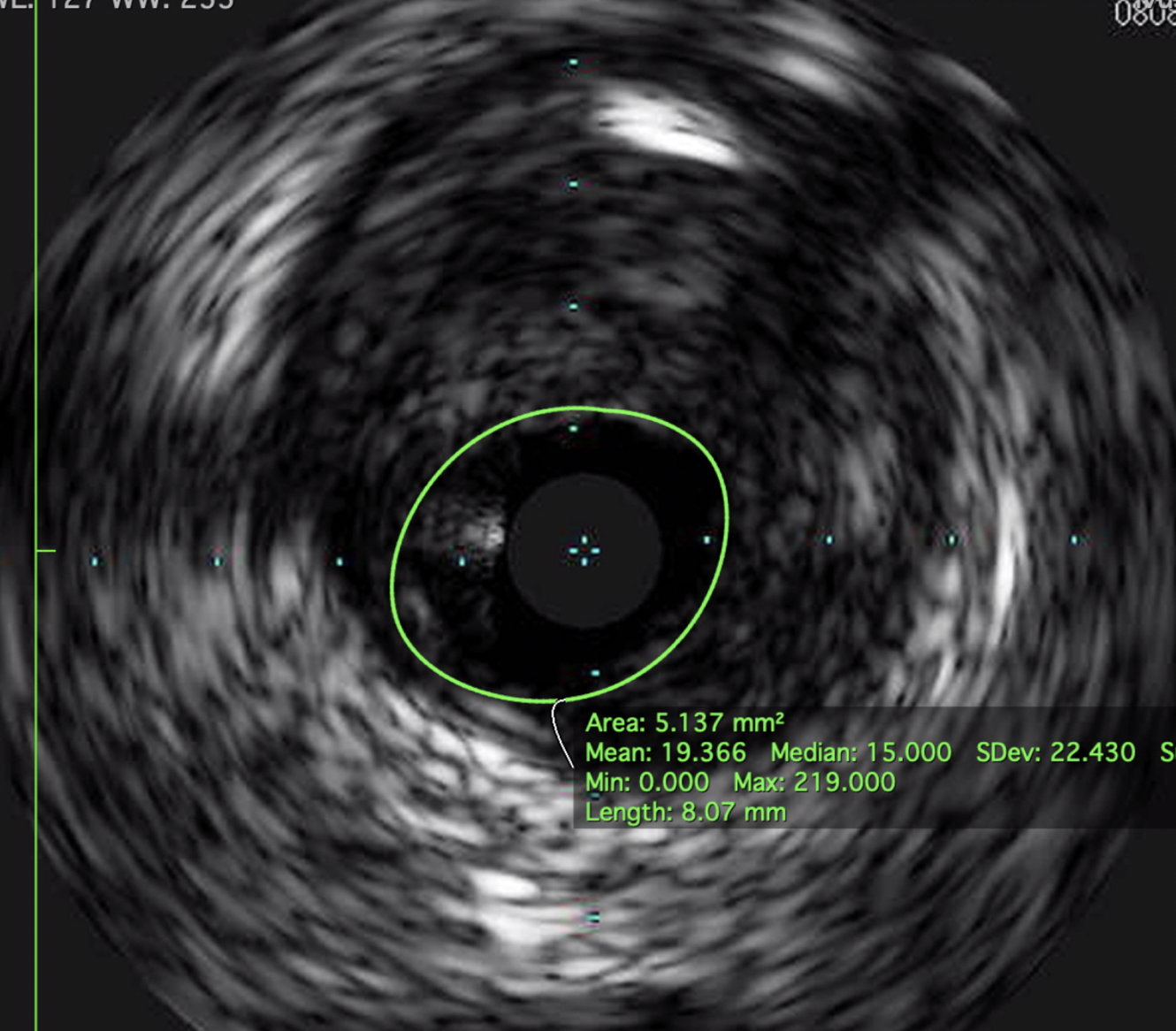
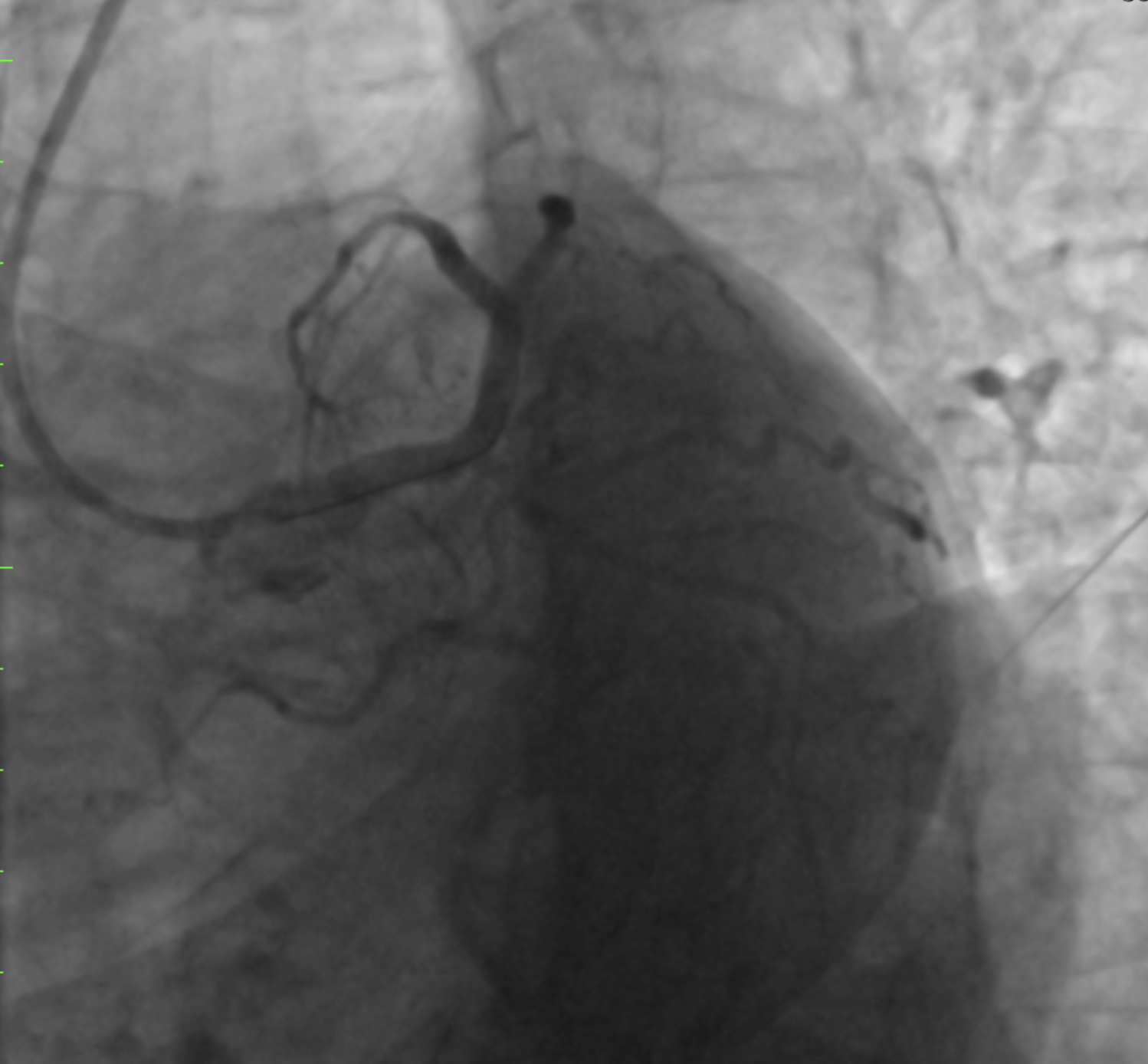
In our patient, IVUS was performed and showed significant stenosis at distal LM with minimum lumen area of 5.13 mm2 (Figure 3). The patient was referred to the heart team for consideration of CABG. With input from the patient and family, and considering his advanced age, the heart team, the patient, and his family declined CABG. He underwent PCI with stenting of both LM and LAD-diagonal bifurcation lesions, yielding a satisfactory result (Figures 4-5).
Figure 3
Figure 3
Figure 4
Figure 4
Figure 5
Figure 5
References
Fearon WF, Yong AS, Lenders G, et al. The impact of downstream coronary stenosis on fractional flow reserve assessment of intermediate left main coronary artery disease: human validation. JACC Cardiovasc Interv 2015;8:398-403.
Ramadan R, Boden WE, Kinlay S. Management of Left Main Coronary Artery Disease. J Am Heart Assoc 2018;7:e008151.