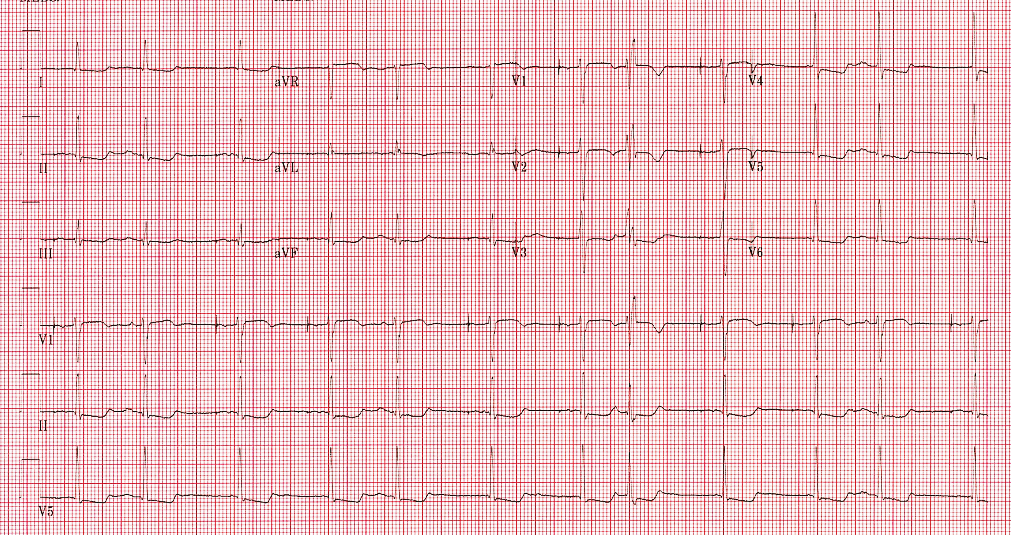
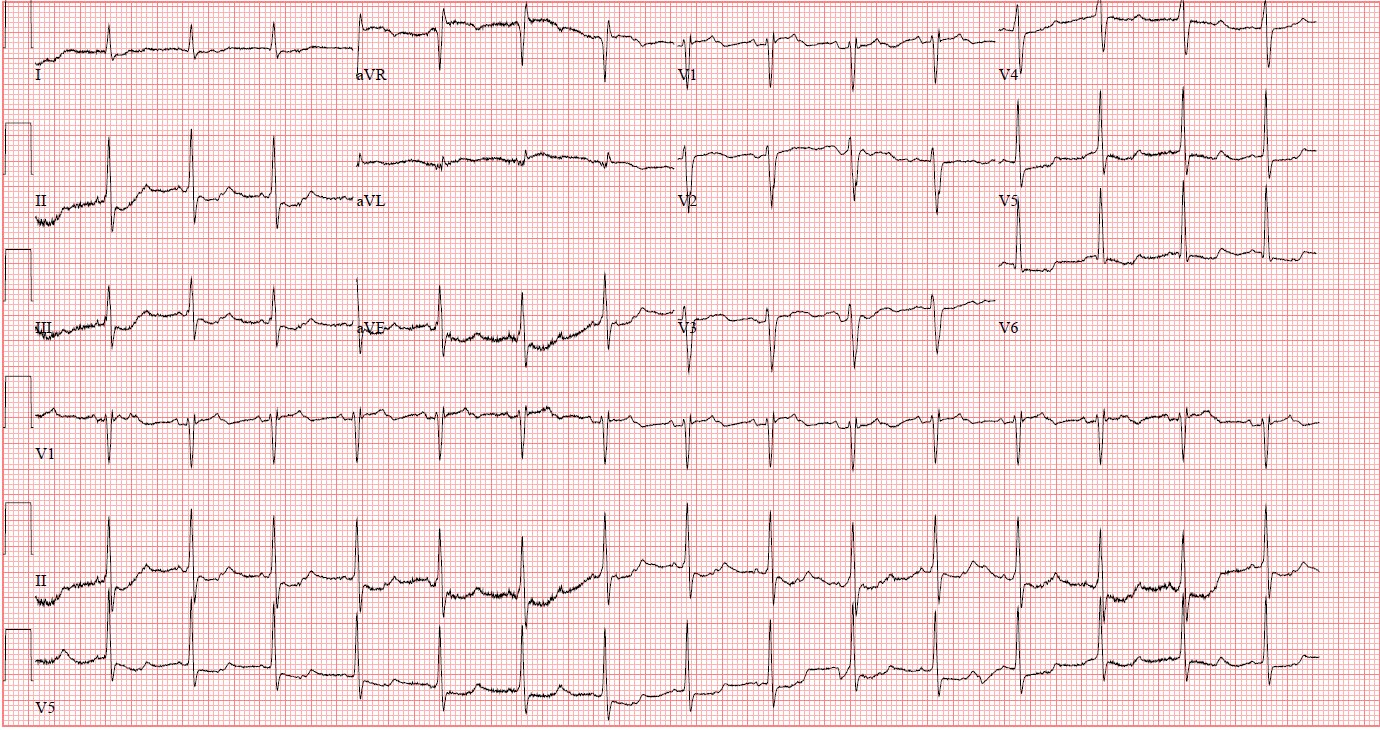
This is 80-year-old male with a history of coronary artery disease, s/p coronary artery bypass grafting, type II diabetes, hypertension, hyperlipidemia and paroxysmal atrial fibrillation. The patient recently had a dual-chamber pacemaker placed for symptomatic sinus bradycardia. Patient was seen in clinic and noted to have palpitations and chest pain. An ECG was obtained at the time of his clinic visit (A). An ECG prior to pacemaker placement is included for comparison (B).
A
Figure A
B
Figure B
The ECG obtained in clinic (A) shows which of the following:
Show Answer
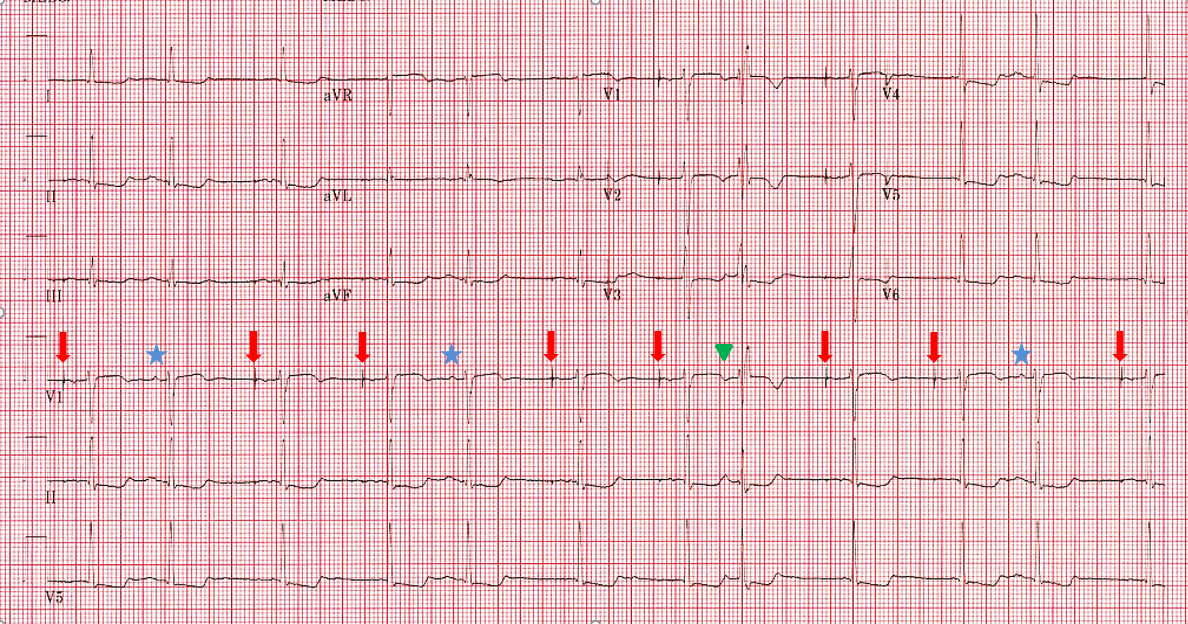
The correct answer is: C. Atrial paced rhythm, sinus rhythm, aberrantly conducted PAC.
The first step to answering this question is determining the atrial activity. It is important to look at the P-wave in all leads when asking this question. Pacing spikes may be seen in one lead but not others depending on position and type of lead, polarity of leads, and placement of ECG patches.1 In this case there are atrial pacing markers most noticeable in lead VI and V2 (arrows), therefore the answer must be either B, C, or D. Examining these remaining options necessitates a clear understanding for the initiation of the remaining complexes that appear in this ECG. Specifically, one must determine which combination of the following is present: sinus rhythm, PACs and PVCs.
Perhaps the best way to do this is to move across the rhythm strip in V1 (where atrial pacing spikes are clearly seen) and examine the atrial activity. The second QRS complex is initiated by a P-wave indicated by a blue star. This same P wave is noted to be present in the 5th and 11th QRS complexes. How do we determine if this is a PAC or sinus rhythm? Obtaining the ECG while the patient is in sinus rhythm allows for the comparison of the P-wave morphology to that in sinus rhythm. ECG B shows a similar P-wave morphology in V1. Furthermore, the P-wave axis is similar to that in sinus rhythm: biphasic in V1, and positive in II, III, aVF. Therefore, these P-waves are likely coming from the sinus node.
In comparison, the P-wave marked with a green triangle that proceeds the 8th QRS complex is a different morphology and noticeably wider. In addition, the P-wave axis is significantly different: negative in V1 and V2, but positive in II, V3 and V5. This P-wave is much earlier than any other P-wave on the tracing in relation to the previous QRS complex and therefore a premature atrial complex.
This QRS complex is in a right bundle branch block (RBBB) morphology and an illustration of Ashman's Phenomenon. There is aberrant ventricular conduction of RBBB morphology as a result of relatively long, followed by a relatively short cycle length. A right bundle branch pattern is typically seen given the longer refractory period of the right bundle branch.2 Therefore, the correct answer is C: the 8th beat (green triangle) is an aberrantly conducted PAC rather than a PVC.
Figure C
References
Bereuter L, Gysin M, Kueffer T, et al. Leadless dual-chamber pacing: a novel communication method for wireless pacemaker synchronization. JACC Basic Transl Sci 2018;3:813–23.
Fisch C. Electrocardiography of arrhythmias: from deductive analysis to laboratory confirmation–twenty-five years of progress. J Am Coll Cardiol 1983;1:306-16.