A 48-year-old female lawyer from South Africa presents for an opinion regarding her management following a complicated course of intractable recurrent pericarditis. Her medical history also includes mitral valve prolapse with mild mitral regurgitation, steroid-induced glaucoma, cataracts, gastritis, osteoporosis, and kidney stones. The patient is an athlete and exercises four to five times weekly.
She was first diagnosed with pericarditis two years ago. She had a delayed diagnosis after a 3-month prodrome of diarrhea, cough and dyspnea with elevated Coxsackie B antibody titers. One month later, she developed typical pleuritic chest pain, high grade fever, and a small pericardial effusion on computed tomography of the chest. She was diagnosed with viral pericarditis and started first on diclofenac 75 mg orally twice daily, and later on prednisone 30 mg once daily and colchicine 0.6 mg once daily. Cardiac magnetic resonance imaging of the heart showed increased pericardial signal on delayed enhancement sequences and an increased pericardial thickness confirming active pericarditis. She underwent endomyocardial biopsies due to persistent disease, which showed active inflammation consistent with myopericarditis, without evidence of any specific secondary causes (Figure 1).
Figure 1
Figure 1
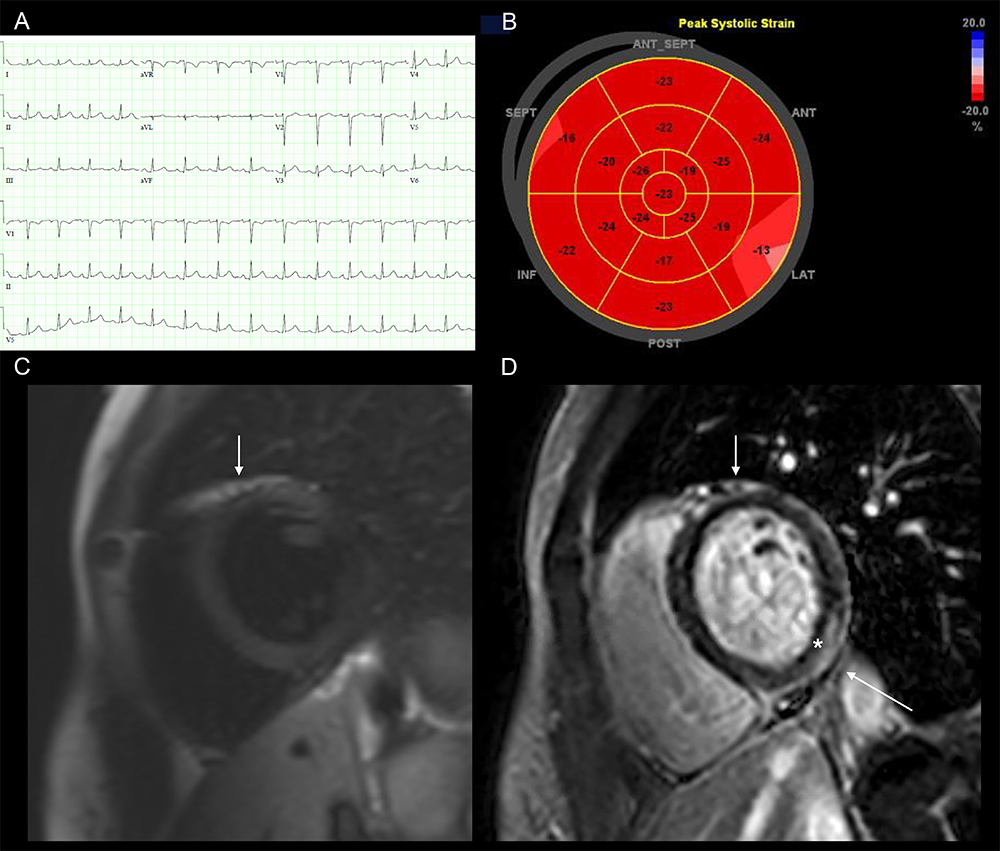
Figure 1: (A) Electrocardiogram with subtle ST elevation and PR-depression confined to the inferior limb leads. (B) longitudinal 2D speckle tracking Bull's eye plot, demonstrating abnormal strain values in the basal infero-lateral segment. (C) Short axis CMR T2-STIR imaging showing increased pericardial (arrow) signals within the anterior and anteroseptal segments. (D) Short axis CMR delayed sequences after injection of gadolinium contrast agent showing increased myocardial (*) and pericardial (arrow) signals within the mid-inferior and inferolateral segments. This constellation of findings is consistent with peri-myocarditis.
Figure 1: (A) Electrocardiogram with subtle ST elevation and PR-depression confined to the inferior limb leads. (B) longitudinal 2D speckle tracking Bull's eye plot, demonstrating abnormal strain values in the basal infero-lateral segment. (C) Short axis CMR T2-STIR imaging showing increased pericardial (arrow) signals within the anterior and anteroseptal segments. (D) Short axis CMR delayed sequences after injection of gadolinium contrast agent showing increased myocardial (*) and pericardial (arrow) signals within the mid-inferior and inferolateral segments. This constellation of findings is consistent with peri-myocarditis.
The initial episode resolved, however, she had multiple recurrences on resumption of her exercise program with incessant pericarditis despite aggressive therapy with more than ten emergency room presentations and hospitalizations. Because of her inability to wean down steroids, she was tried on multiple immunosuppressive medications: intravenous immune globulin, intrapericardial instillation of corticosteroids, azathioprine, methotrexate, and finally, anakinra. With these treatments she developed significant adverse effects including fungal and bacterial esophagitis (methotrexate), Stevens-Johnson syndrome (anakinra), and steroid-induced glaucoma, cataracts, and osteoporosis.
Eight years after her initial episode, she was still having recurrent bouts of pericarditis despite restriction from exercise and medication regimen of methylprednisolone 6 mg daily, meloxicam 15 mg daily and aspirin 250 daily. She ultimately decided to undergo radical pericardiectomy at a center with specific expertise in this surgery. The entire pericardium was removed to the level of the oblique sinus and the patient's symptoms resolved until this day.
Which of the following is true regarding the treatment approach for patients with recurrent pericarditis?
Show Answer
The correct answer is: E. Exercise restriction is still recommended in acute and recurrent pericarditis, although little data exist regarding its benefit.
This athletic patient had recurrent viral pericarditis with the resumption of her exercise program. Her pericarditis ultimately became resistant to colchicine, steroids, and immunosuppressive medications, and she eventually required a pericardiectomy to treat her condition.
Although there is little conclusive data regarding its benefit, exercise restriction is still recommended in the most recent society guidelines.1 It is recommended that activity be restricted to the minimal exertion necessary for routine daily activities and a sedentary profession.2
- As by the position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology, athletes with pericarditis should refrain from exercise for at least 1 to 3 months, depending on the severity of their episode (Class III, level of evidence C). A longer period of time (3 to 6 months) might be needed if there is myocardial involvement as well. It is considered safe to resume exercise if the inflammatory markers have normalized and no ventricular dysfunction or arrhythmias are detected (Class IIa, level of evidence C).3 An isolated asymptomatic pericardial effusion in an athlete is not an indication for activity restriction.
- Regarding non-athletes, the 2015 European Society of Cardiology (ESC) Guidelines for the Diagnosis and Management of Pericardial Diseases, there is no specific time period for activity restriction; normal activity can be resumed with resolution of symptoms and no evidence of active pericarditis (normal inflammatory markers and resolution of echocardiographic and electrocardiographic findings) (Class IIa, level of evidence C).1
Further studies are needed to ascertain the benefit of exercise restriction in both athletes and non-athletes.
While the use of colchicine in the treatment of pericarditis is consider "off-label", colchicine is recommended for all episodes of pericarditis, and is first-line treatment along with non-steroidal anti-inflammatory drugs (NSAIDs). It can be given as 0.6 mg once or twice daily with or without a loading dose. For initial episode it is recommended to treat for 3 months and recurrent episodes the recommendation is for 6 months of therapy. The efficacy of colchicine has been demonstrated in three randomized controlled trials. In these trials, patients were randomized to receive traditional therapy (aspirin, NSAIDs, or steroids) alone or in combination with colchicine. Reliably the addition of colchicine led to reduction in both recurrence of pericarditis and reduction of symptoms at 72 hours. There was no increase of adverse events.4-6 Similarly, there have been two systemic reviews showing the efficacy of colchicine in reducing the recurrence of pericarditis without increase in adverse effects related to colchicine therapy.7,8 Colchicine is generally well-tolerated with gastrointestinal side effects being most prevalent. It may be prescribed in two daily doses rather than one for improved tolerance and compliance.
After failure of first line treatment, steroids should be started as second line therapy at a low dose of 0.2 to 0.5 mg/kg/day and very slowly weaned off over several months.1 A quicker taper has been shown to increase the risk of recurrence and a higher dose of steroids carry no benefit with the additional burden of side effects, as seen in our patient.9 If steroids are unable to be weaned without recurrence, immunosuppressive medications should be tried. Novel immunomodulators, specifically those blocking Interleukin-1, such as rilonacept, anakinra and canakinumab, have been proven effective and safe.10-12
Pericardiectomy is an imperfect and unpredictable therapy which should be considered in patients that have failed medical therapy and continue to have relapsing pericarditis. The ESC recommends pericardiectomy as a last option for those with pericarditis refractory to all medical therapies.1 This therapy should only be considered at tertiary referral centers with expertise in this procedure. Comparison of surgical and medical therapies has shown no difference in regard to mortality between the groups, however there was a reduction in pericarditis recurrence rate for patients treated with surgical pericardiectomy. There is a trend toward less medication use, particularly less use of corticosteroids, in patients treated surgically with pericardiectomy.13
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases. Eur Heart J 2015;36:2921-64.
Pelliccia A, Solberg EE, Papadakis M, et al. Recommendations for participation in competitive and leisure time sport in athletes with cardiomyopathies, myocarditis, and pericarditis: position statement of the Sport Cardiology Section of the European Association of Preventive Cardiology (EAPC). Eur Heart J 2019;40:19-33.
Imazio M, Brucato A, Cemin R, et al. Colchicine for Recurrent Pericarditis (CORP). Ann Intern Med 2011;155:409-14.
Imazio M, Bobbio M, Cecchi E, et al. Colchicine as first-choice therapy for recurrent pericarditis: results of the CORE (COlchicine for REcurrent pericarditis) trial. Arch Intern Med 2005;165:1987-91.
Imazio M, Belli R, Brucato A, et al. Efficacy and safety of colchicine for treatment of multiple recurrences of pericarditis (CORP-2): a multicentre, double-blind, placebo-controlled, randomised trial. Lancet 2014;383:2232-37.
Imazio M, Brucato A, Forno D, et al. Efficacy and safety of colchicine for pericarditis prevention. Systematic review and meta-analysis. Heart 2012;98:1078-82.
Alabed S, Cabello JB, Irving GJ, Qintar M, Burls A. Colchicine for pericarditis. Cochrane Database Syst Rev 2014;28:CD010652.
Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation 2008;118:667-71.
Lazaros G, Antonatou K, Vassilopoulos D. The therapeutic role of interleukin-1 inhibition in idiopathic recurrent pericarditis: current evidence and future challenges. Front Med 2017;4:78.
Van Tassell BW, Toldo S, Mezzaroma E, Abbate A. Targeting interleukin-1 in heart disease. Circulation 2013;128:1010-23.
Klein A, Lin D, Cremer P, et al. Rilonacept in recurrent pericarditis: first efficacy and safety data from an ongoing phase 2 pilot clinical trial. J Am Coll Cardiol 2019;73:1261.
Khandaker MH, Schaff HV., Greason KL, et al. Pericardiectomy vs medical management in patients with relapsing pericarditis. Mayo Clin Proc 2012;87:1062-70.