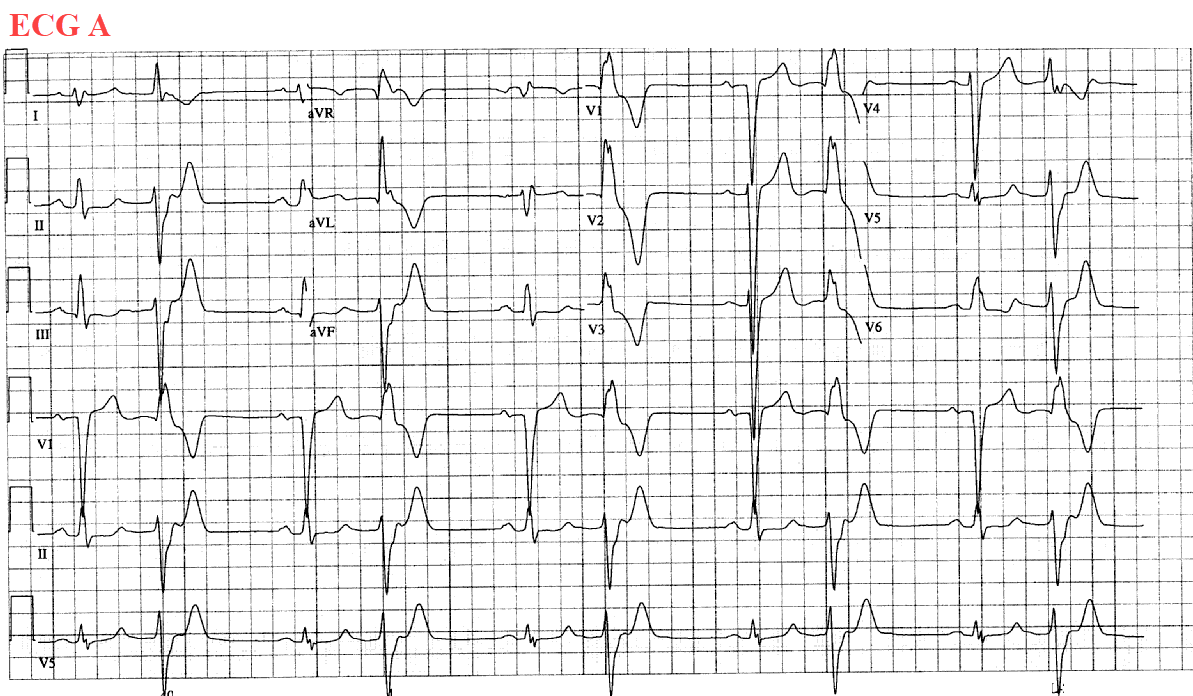
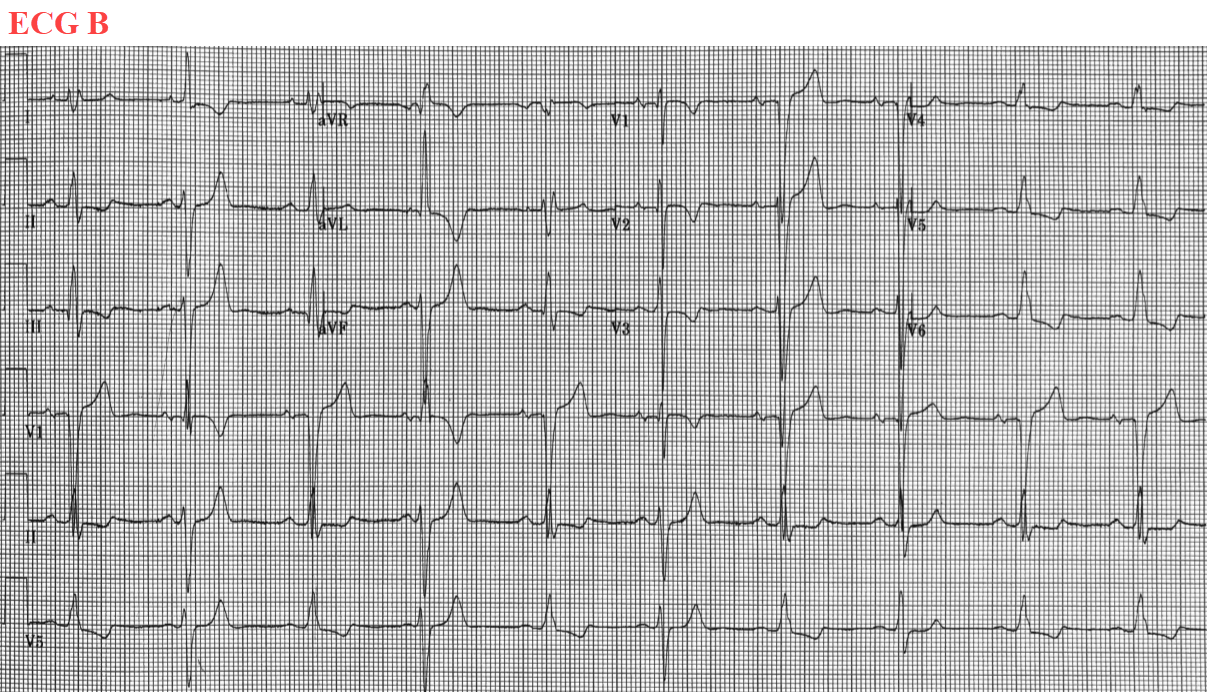
A 91-year-old woman with a past medical history of remote coronary artery bypass surgery, hypertension, and hyperlipidemia, presented for evaluation of frequent premature ventricular contractions (PVCs) in the setting of a declining left ventricular ejection fraction. She was started on amiodarone for the PVCs that are depicted on "ECG A." She then presented back to our clinic one year later with a chief complaint of fatigue. The ECG from this clinic visit is depicted as "ECG B."
ECG A
ECG B
ECG B is most consistent with which of the following:
Show Answer
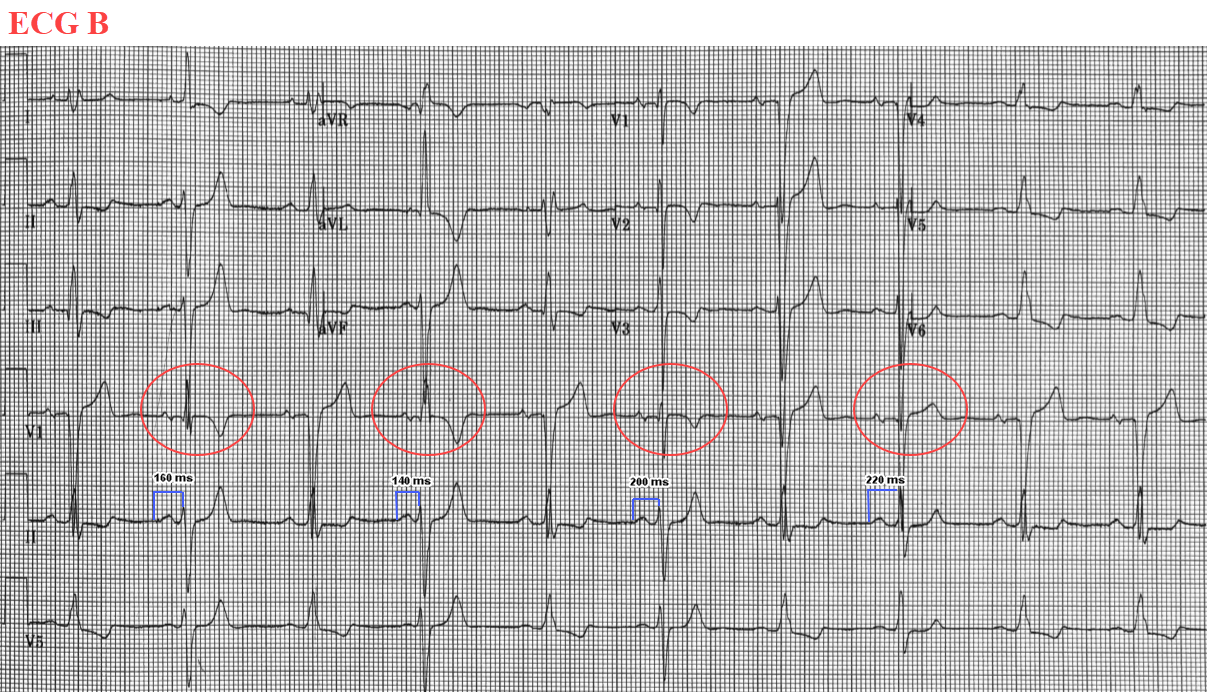
The correct answer is: C. Sinus rhythm with fusion complexes.
In ECG A, PVCs are present with a right-bundle branch block morphology, negative QRS deflection in limb leads II, III, aVF and positive QRS deflection in leads I and aVL. This PVC is likely originating from the posteromedial papillary muscle in the left ventricle. Furthermore, there are no P-waves prior to the PVCs. ECG B is interesting in that P-waves are seen before every QRS complex at a rate of 60 bpm. These P-waves are sinus in origin and do not occur early (option A is incorrect). The patient has variable degree of fusion beats on ECG B which are encircled in red. We know that her prior PVCs were of a right bundle branch block morphology. The morphology of these QRS complexes are all unique due to a varying degree of fusion ventricular myocardial depolarization through the His-Purkinje system and PVC. Her baseline PR interval is 240 ms and with shorter PR intervals there is a greater contribution to ventricular depolarization from the PVC as opposed to the native conduction through the His-Purkinje system. This results in QRS complexes that appear closer in morphology to her known PVCs because her sinus impulse has not had enough time to conduct down to the His-Purkinje system before her ventricular myocardium has been depolarized by the PVC. The corollary is also true, when the patient's PR interval is closer to 240 ms, the patient's QRS complexes appear like her native QRS complexes owing to more contribution from myocardial depolarization through her His-Purkinje system. Rather than these being multifocal PVCs, her ECG is more consistent with varying degrees of QRS fusion (making option B less likely). Finally, option D is unlikely as intermittent preexcitation is usually seen with premature atrial impulses rendering the AV node more refractory (i.e., less "slick"), forcing conduction down an accessory pathway; however, the patient has a consistent sinus rhythm and no PACs.
ECG B
References
Al'Aref SJ, Ip JE, Markowitz SM, et al. Differentiation of papillary muscle from fascicular and mitral annular ventricular arrhythmias in patients with and without structural heart disease. Circ Arrhythm Electrophysiol 2015;8:616-24.
Greenstein E, Goldberger JJ. Implications of progressive aberrancy versus true fusion for diagnosis of wide complex tachycardia. Am J Cardiolo 2011;108:52-5.