A 61-year-old man with a history of obstructive sleep apnea, paroxysmal atrial fibrillation and dilated non-ischemic cardiomyopathy was admitted to the hospital for orthotopic heart transplantation. His preoperative left ventricular ejection fraction was 15% and left ventricular end-diastolic diameter was 7.2 cm. The patient's body mass index was 28 kg/m2. The body mass index of the donor was unknown. Serologies showed that both the donor and recipient were positive for prior cytomegalovirus and Epstein-Barr virus antibodies.
The patient underwent an uncomplicated heart transplant surgery with bicaval anastomosis technique. The donor heart's cold ischemic time was 201 minutes. Methylprednisolone and basiliximab were given for immunosuppression induction, followed by a maintenance immunosuppression regimen of mycophenolate mofetil 1g twice daily and prednisone 20mg once daily. Tacrolimus was added nine days after transplantation. Trimethoprim-sulfamethoxazole and valganciclovir were given for antimicrobial prophylaxis.
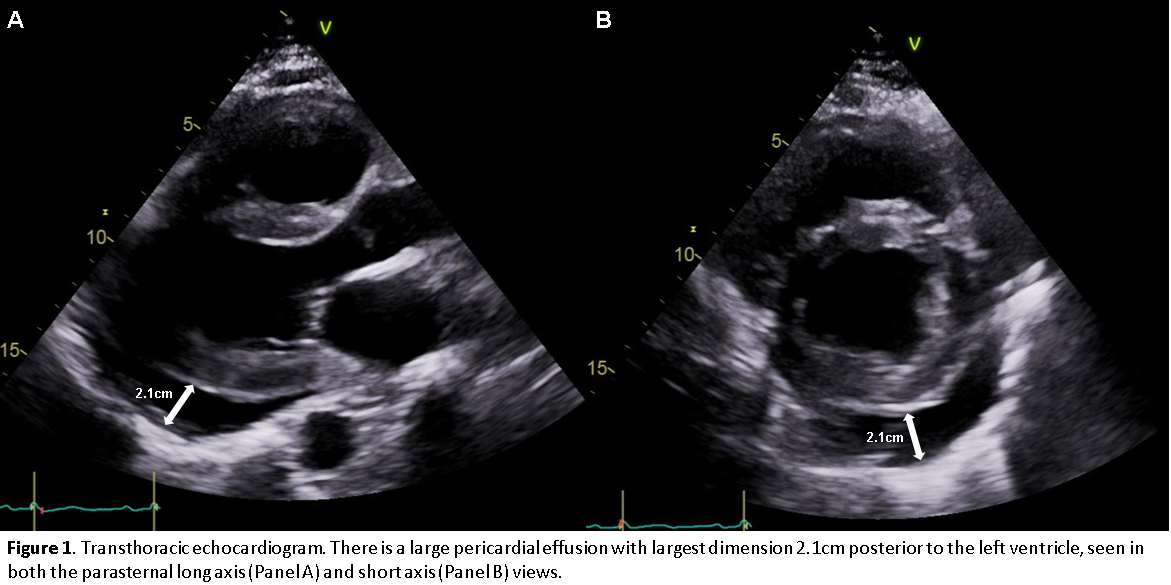
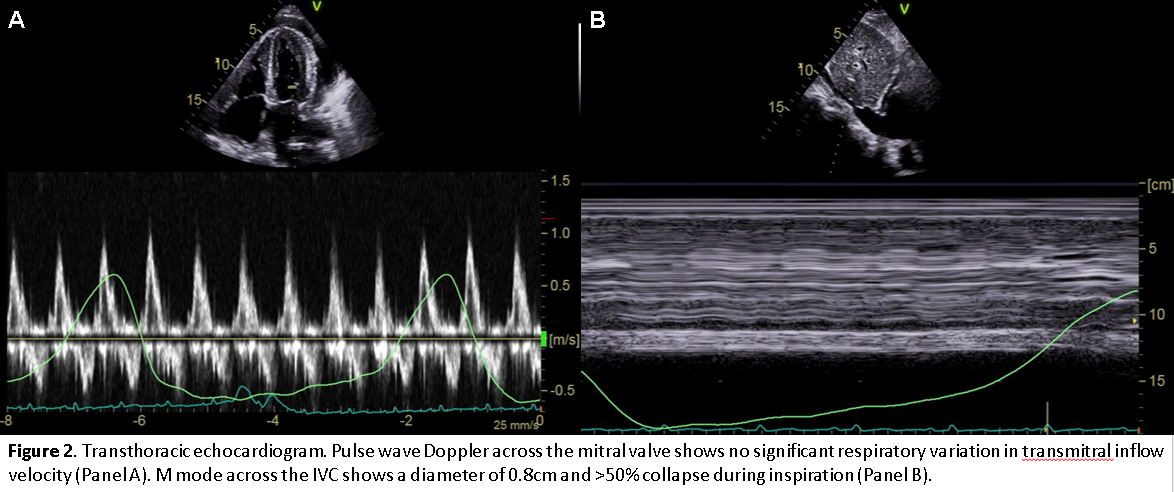
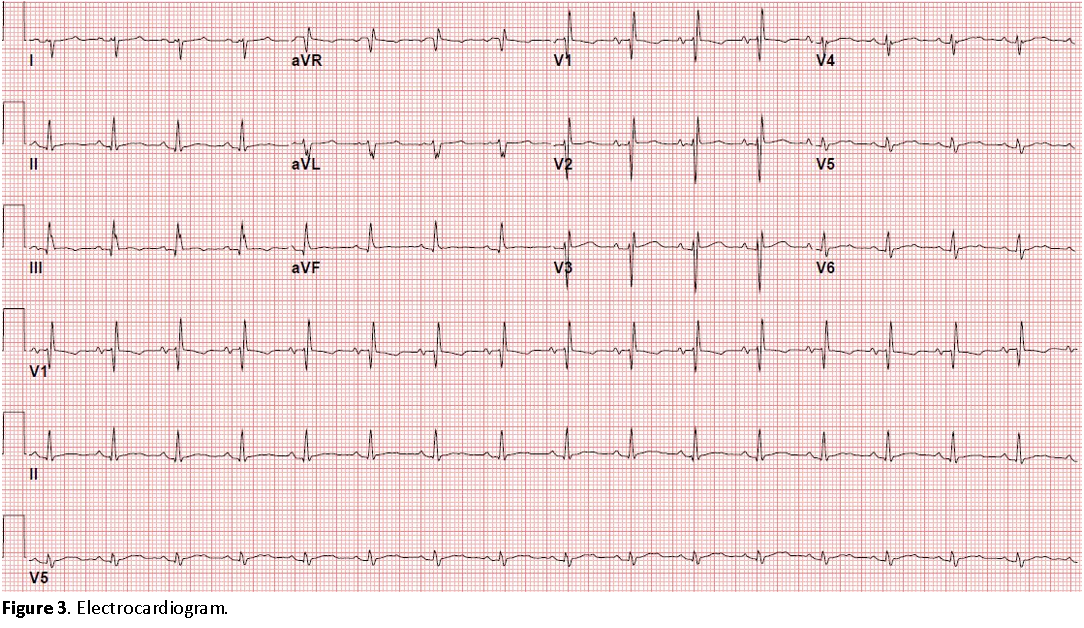
A surveillance endomyocardial biopsy performed ten days after transplantation showed evidence of moderate acute cellular rejection (grade 2R). An echocardiogram performed on the same day (prior to the endomyocardial biopsy) showed a large concentric pericardial effusion, with greatest dimension 2.1cm posterior to the left ventricle (Figure 1). There was no diastolic chamber collapse and no significant respiratory variation in the mitral and tricuspid inflow velocities (Figure 2A). The inferior vena cava diameter was 0.8cm with collapse >50% during inspiration (Figure 2B). Left and right ventricular size and function were normal. The patient was asymptomatic with temperature 97.9 °F, blood pressure 113/69 mmHg, heart rate 86 beats per minute, respiratory rate 16 breaths per minute, and peripheral oxygen saturation 98%. Electrocardiogram is shown in Figure 3. Laboratory studies were notable for creatinine 1.0, white blood cell count 6,000/mm3, hemoglobin 10.0 g/dL, platelet count 446,000/mm3, and international normalized ratio 1.2.
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
Which of the following is the best next step in management of this patient?
Show Answer
The correct answer is: C. Increase prednisone dose and repeat echocardiogram in one week.
Pericardial effusions are common following orthotopic heart transplantation, with retrospective studies reporting moderate to large pericardial effusions in 6% to 35% of patients.1-6 This rate is similar to that reported for a general cardiac surgery population.7 Most post-transplant effusions are detected early after surgery, with the average time to detection ranging from 12 to 20 days. The development of cardiac tamponade in this setting is uncommon, occurring in 3% to 8% of patients with moderate to large effusions.
Patients undergoing orthotopic heart transplantation are at risk for the development of pericardial effusions due to usual causes after cardiac surgery as well as transplant-specific causes. The most well recognized causes of pericardial effusion following cardiac surgery are pericardial hemorrhage and postpericardiotomy syndrome. In the post-transplant population, retrospective studies have identified several unique risk factors associated with the development of pericardial effusions in the early post-operative period. These risk factors include the use of sirolimus, prolonged donor heart ischemic time, donor-recipient weight mismatch, and the absence of prior cardiac surgery. Right ventricular perforation during endomyocardial biopsy must also be considered as a cause of a hemorrhagic pericardial effusion in this population.
The exact mechanism by which sirolimus is associated with development of a pericardial effusion is not known,8 but it is notable that the association between sirolimus and pericardial effusions has also been observed in patients receiving other types of organ transplant.9,10 Cyclosporine has also been cited as a possible cause of pericardial effusion;1,11 however, the evidence supporting this association is less robust. One retrospective study has demonstrated an increase in donor heart ischemic time in patients who developed an early post-transplant pericardial effusion compared to patients who did not develop an effusion (180 ± 59 min vs. 147 ± 52 min).6 Ischemia-reperfusion injury has been proposed as a mechanism that might explain this finding. In the case of donor-recipient weight mismatch, it is theorized that a simple hydrostatic gradient may promote the development of a pericardial transudate in a recipient that is of greater weight (and with an assumed larger pericardial cavity) than the donor.3 The protective effect of prior cardiac surgery against the development of a pericardial effusion has been demonstrated in multiple studies and may be related to preexisting pericardial adhesions and scar.3-5 Notably, while initial studies of post-transplant patients suggested an association between acute rejection and postoperative pericardial effusions,2,4 more recent studies have not supported this finding.5,6
Most pericardial effusions following heart transplantation are benign and resolve with time. For example, in one retrospective study of 88 post-transplant patients, 31 (35%) developed a pericardial effusion, all of which resolved within three months of follow up.6 Therefore, in the absence of cardiac tamponade or a clearly treatable cause for a post-transplant pericardial effusion, management generally consists of periodic follow up echocardiograms to monitor the size of the effusion. In some cases, pericardial effusions may enlarge or recur, in which case pericardiocentesis or a pericardial window may be required for symptomatic relief and prevention of recurrence. In this case, special attention should be given to potential untreated causes of the pericardial effusion, such as continued sirolimus therapy or post-pericardiotomy syndrome requiring more intense immunosuppression.
The patient in this case has an asymptomatic, large pericardial effusion with no clinical or echocardiographic evidence of cardiac tamponade. Therefore, pericardial drainage is not necessary. He has no fever, pleuritic chest pain or electrocardiographic evidence of pericarditis to suggest post-pericardiotomy syndrome. As such, treatment with colchicine and a non-steroidal anti-inflammatory drug is not indicated. While he does have moderate acute cellular rejection, it is unclear whether rejection is associated with the development of pericardial effusions. Ultimately, this patient's pericardial effusion was attributed to a relatively long donor heart ischemic time and possible donor-recipient size mismatch. He was started on prednisone 100mg daily for three days as treatment for his acute cellular rejection. Mycophenolate mofetil and tacrolimus were continued. A repeat echocardiogram one week later showed a significant decrease in size of the pericardial effusion to 0.8cm in maximum dimension, which was unchanged on another echocardiogram performed four months later. An echocardiogram performed one year post-transplant showed complete resolution of the pericardial effusion, and surveillance endomyocardial biopsies showed no further evidence of rejection.
References
Vandenberg BF, Mohanty PK, Craddock KJ, et al. Clinical significance of pericardial effusion after heart transplantation. J Heart Transplant 1988;7:128-34.
Valentine HA, Hunt SA, Gibbons R, Billingham ME, Stinson EB, Popp RL. Increasing pericardial effusion in cardiac transplant recipients. Circulation 1989;79:603-9.
Hauptman PJ, Couper GS, Aranki SF, Kartashov A, Mudge GH Jr, Loh E. Pericardial effusions after cardiac transplantation. J Am Coll Cardiol 1994;23:1625-9.
Ciliberto GR, Anjos MC, Gronda E, et al. Significance of pericardial effusion after heart transplantation. Am J Cardiol 1995;76:297-300.
Quin JA, Tauriainen MP, Huber LM, et al. Predictors of pericardial effusion after orthotopic heart transplantation. J Throac Cardiovasc Surg 2002;124:979-83.
Al-Dadah AS, Guthrie TJ, Pasque MK, Moon MR, Ewald GA, Moazami N. Clinical course and predictors of pericardial effusion following cardiac transplantation. Transplant Proc 2007;39:1589-92.
Pepi M, Muratori M, Barbier P, et al. Pericardial effusion after cardiac surgery: incidence, site, size, and haemodynamic consequences. Br Heart J 1994;72:327-31.
Keogh A, Richardson M, Ruygrok P, et al. Sirolimus in de novo heart transplant recipients reduces acute rejection and prevents coronary artery disease at 2 years: a randomized clinical trial. Circulation 2004;110:2694-700.
Steele GH, Adamkovic AB, Demopoulos LA, et al. Pericardial effusion coincident with sirolimus therapy: a review of Wyeth's safety database. Transplantation 2008;85:645-7.
Holbro A, Ahmad I, Busque L, et al. Cardiac tamponade potentially related to sirolimus following cord blood transplantation. Bone Marrow Transplant 2012;47:294-5.
Hastillo A, Thompson JA, Lower RR, Szentpetery S, Hess ML. Cyclosporine-induced pericardial effusion after cardiac transplantation. Am J Cardiol 1987;59:1220-2.