

Career Challenges of the SHD Imager
Structural heart disease (SHD) imaging is a new and evolving paradigm in cardiac imaging. Its primary components are echocardiography and cardiac computed tomography, with a focus on preprocedural planning and intraprocedural guidance of noncoronary transcatheter heart therapies.
SHD imaging is among the most exciting and rewarding subspecialties within cardiology and is critical to the success of the procedures. However, the SHD imaging community continues to face significant challenges that threaten its growth and quality.
Training
New Trainees
Although the number of hospitals performing transcatheter structural heart interventions continues to increase, the number of qualified SHD imagers remain few. SHD imaging training in general cardiology fellowships is limited. Cardiac imaging is the only unaccredited subspecialty within cardiology.
One consequence of this is significant variability of the requisite multimodality imaging training between institutions. Additionally, few imaging fellowships offer sufficient training. Although some groups have proposed metrics for training, no SHD imaging training guidelines have been published to date.
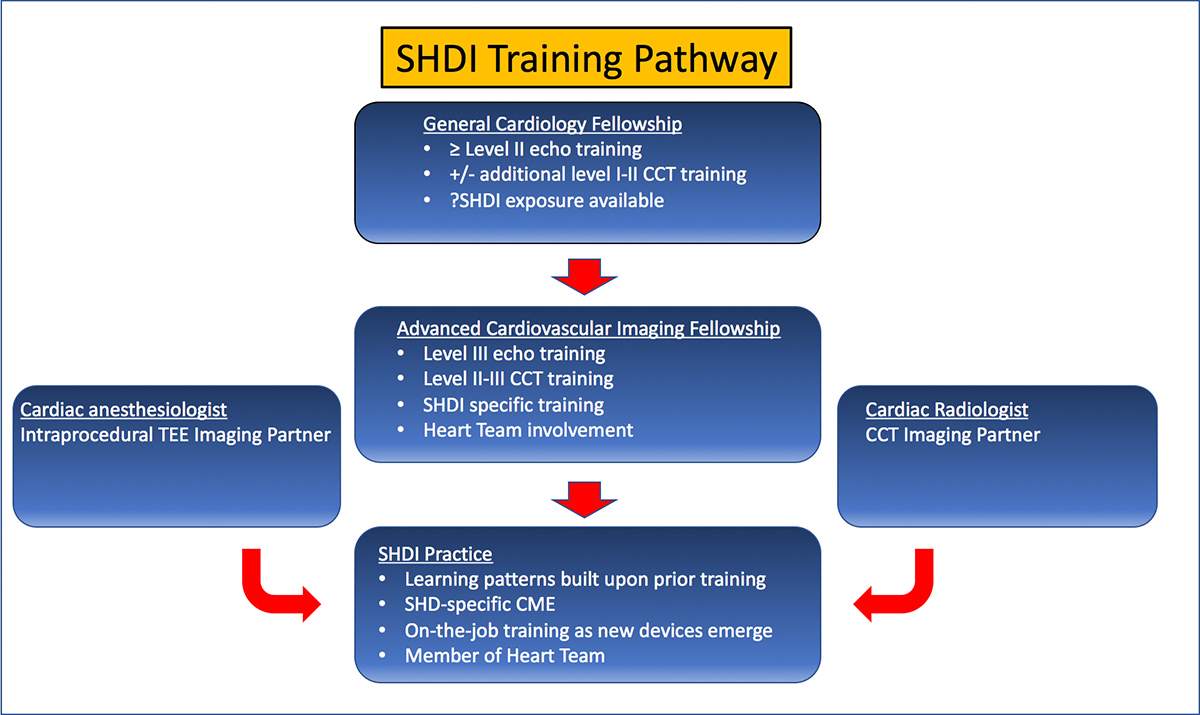
A recent AATS/ACC/SCAI/STS consensus document has proposed operator and institutional requirements, but further guidance on SHD imaging training is needed (Figure 1). A very robust training program must imbue the seeds which will blossom into on-the-job CME as a multitude of new devices and procedures become available.
Figure 1. Sample training pathway for the SHD imager
Practicing Physicians
For those in already practice, the opportunities to learn are generally limited to industry training courses, society training courses, review of the literature, local proctoring or a mini-fellowship type of experience at an SHD imaging center. It is often difficult to achieve competency with these options alone in a busy clinical practice and further avenues are needed.
Transition From Training to Practice
Although the demand for a SHD imager is high, obstacles remain for early career growth. In the age of the relative value units (RVUs), SHD imagers are plagued by disproportionately low reimbursement for their services. The large amount of time required to plan and guide procedures is not reflected in RVUs earned for cardiac computed tomography or intraprocedural transesophageal echocardiography.
For example, despite the important role of the echocardiographer as the co-operator in Mitraclip implantation, the SHD interventionalist is reimbursed approximately 10 times the revenue of the SHD imager. Without a revenue sharing model, the SHD imager will constantly fall short of RVU targets despite high workload.
Attempts to make up for these deficiencies through other RVU-generating duties hinders the SHD imager, curbs academic activity and may lead to physician burnout.
The ACC Imaging Council and SHD imaging workgroup, along with other society workgroups, are leading advocacy efforts to address compensation issues. Existing reimbursement models must change for the SHD imager to thrive.
Wellness
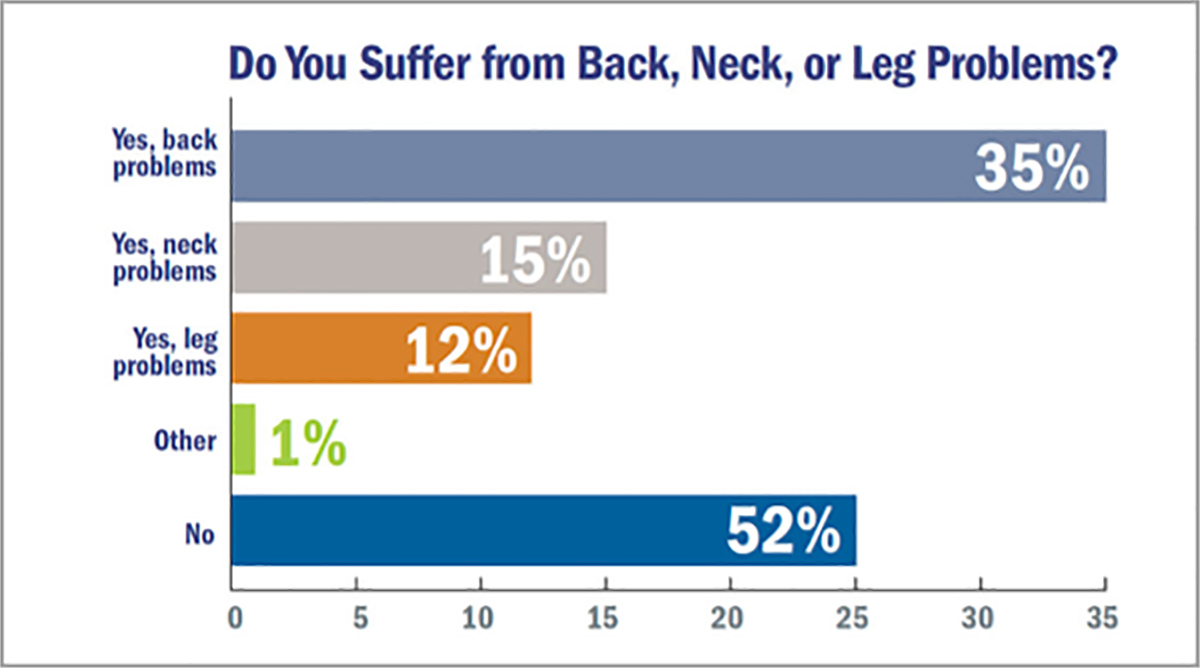
In addition to wellness issues created by inequitable reimbursement models, there are other health concerns associated with SHD imaging. Up to 50 percent of interventional cardiologists have reported suffering from or treatment for orthopedic problems, and a recent CardioSurve survey reported that approximately 50 percent of all cardiologists suffer from some form of orthopedic pain (Figure 2).
Figure 2. CardioSurve survey on orthopedic pain among cardiologists
Steps to maximize ergonomics are crucial to prevent similar morbidity in SHD imagers. Radiation exposure is another pressing concern. Although there have been conflicting data on increased risk of malignancies from occupational radiation exposure, the incidence of cataracts is clearly higher in interventional cardiologists. Recent data have shown that the SHD imager receives at least double the radiation dose of the interventional cardiologist first operator.
While cath lab designs have improved to provide more protection for interventional cardiologists, the shielding for the SHD imagers is still a significant issue. Ongoing education and advocacy focused on these issues is key moving forward.
Future
The future of SHD imaging is bright. It is a key part of the unprecedented innovation and progress in the treatment of SHD. Efforts to promote the careers and wellness of SHD imagers are critical for the future success of the structural heart disease field.


This article was authored by Nadira Hamid, MBChB (@HamidNadira), and Omar K. Khalique, MD, FACC (@OKhaliqueMD), from the Structural Heart and Valve Center, Columbia University Medical Center/NY Presbyterian Hospital in New York, NY.