

Pros and Cons of Pursuing Advanced Training in CCT Without Advanced Cardiac MRI: An Early Career Cardiologist Perspective
Cardiac magnetic resonance (CMR) and cardiac computed tomography (CCT) have revolutionized the cardiac imaging field in large part due to high spatial resolution and three-dimensional capabilities. While achieving level II training in echocardiography and nuclear imaging (SPECT) is frequently achievable within the three-year general cardiology fellowship training, acquiring advanced training (level II or III) in CCT and CMR generally requires at least one additional year of training. This training has significant clinical, academic, social and financial implications on cardiology fellows who are very eager to start their career after long years of training. Training in CCT and CMR has become closely intertwined and many academic centers offer advanced cardiovascular imaging fellowships that train fellows in both CCT and CMR. Such "marriage" between the two modalities has led to the common perception among fellows that one must achieve advanced training in both CCT and CMR.
As an early career cardiologist with advanced training in echocardiography and CCT, but not in CMR, I am frequently asked by my cardiology fellows who are unable to spend a dedicated year in our CMR/CCT lab for advanced imaging fellowship if I would recommend they pursue dedicated level II training in CCT. This article will discuss the advantages and potential disadvantages of acquiring level II training in CCT without pursuing level II CMR training.
Pros:
- Obtaining level II training in CCT is feasible within the three-year period of general cardiology fellowship. The training requirements for CCT and CMR are very different. To achieve level II cardiac MRI, the fellow must have a minimum of three cumulative months of dedicated CMR training. However, most CMR training programs require more than three months. Given the complex CMR physics and an ever-expanding number of pulse sequences including parametric mapping techniques, many will need more than three months of training to feel comfortable as an independent reader. On the other hand, current training requirement for CCT is less time consuming, and at some centers a general cardiology fellow can more easily achieve level II training within the span of a three-year cardiology fellowship (Table 1).
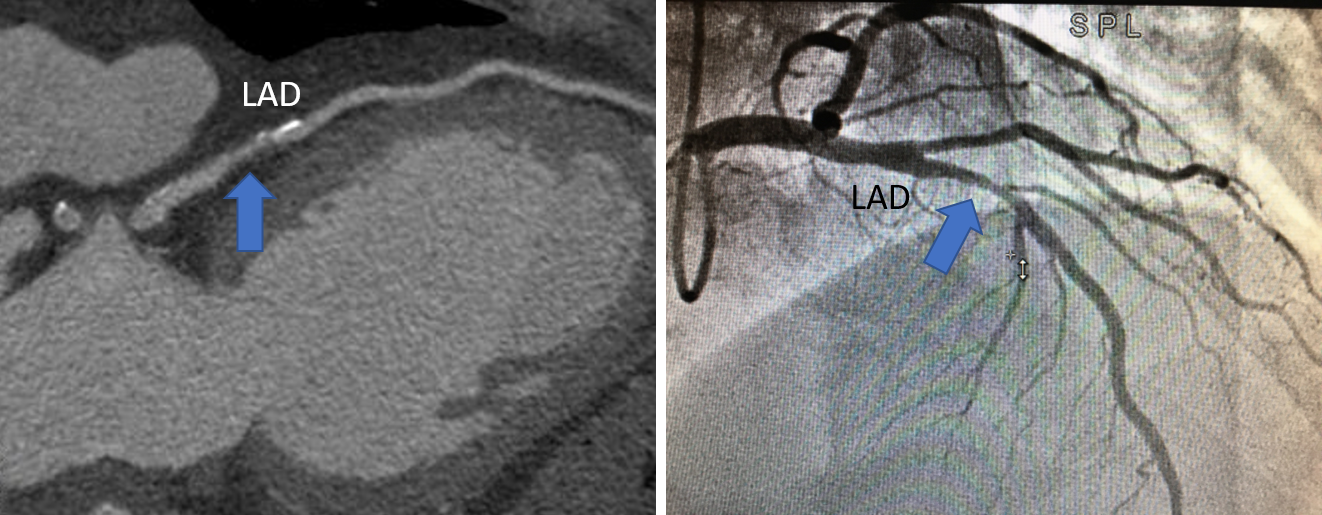
- Learning CCT expands the diagnostic tools of the cardiologist. The clinical applications of CCT such as coronary calcium scanning, coronary CT angiography or CCT for structural heart disease are now routine in daily clinical practice. It is highly advantageous for future cardiologists to be adequately trained in CCT techniques, indications, contraindications, strengths and weaknesses, as well as independent image interpretation. I frequently show my patients images of their coronary calcium score or coronary atherosclerotic lesions to motivate them to adhere to a healthier lifestyle. Furthermore, visualizing the coronary plaque on CCT enhances our understanding of underlying coronary plaque characteristics on invasive coronary angiography. For example, a benign-looking intermediate stenosis of invasive angiogram can be the result of a large size, high-risk plaque on CCT (Figure 1).
- Mastering the CCT technique enhances understanding of other imaging modalities. For example, the large field of view and high spatial resolution of CCT images allows for improved understanding of the context of transthoracic and transesophageal images. For example, 3D imaging the left atrial appendage by CCT pre- and post-percutaneous left atrial appendage occluder (LAAO) device placement allows correlation with transesophageal echocardiography, and improves our understanding of the mechanisms of peri-device leaks and the causes of suboptimal LAAO device positioning.
- Certification in CCT can enhance an academic career. Training in CCT may provide an opportunity for early faculty clinical sub-specialization and a pathway for promotion, as well as opportunities for research ideas that are based on utilizing multiple imaging modalities.
- Certification in CCT can translate into more job opportunities. Many hospitals and academic centers are looking to expand or start a CCT program, and a cardiology fellow with CCT training may have a competitive advantage.
- Simplified scanning protocols of CCT and CMR are frequently capable of providing diagnostic images without much intervention from a level III-trained personnel. Such protocols lead to increase appropriate utilization of CCT and CMR. Subha V. Raman, MD, FACC, director of the CCT/CMR lab at the Ohio State University Medical Center, believes that "with simplified scans to address common clinical questions, CCT and CMR favorably impacts outcomes and practice. Better access to Level II training to both modalities can help deliver this impact to community practices."
Cons:
While there is no real disadvantage for acquiring new knowledge and skills, there are a few challenges and potential hurdles that one should be aware when pursing CCT certification without CMR. These include:
- Inability to practice CCT in daily clinical practice: Many hospitals may not have CCT available or have interest in building a program. When available, many hospitals have their CCT and CMR labs combined, and physicians may be expected to provide coverage for both modalities simultaneously. Therefore, it might be difficult to find a hospital or an academic center where isolated coverage for the CCT lab is needed.
- Persistent need for basic CMR training: Being trained in CCT does not absolve the one from entirely learning CMR. Acquiring level I training in CMR is a necessity for all cardiology fellows as CMR is a very powerful imaging modality with rapidly expanding uses. Familiarity with the modality is essential for any skilled cardiologist in the current era.
- Weak financial incentive: Practicing CCT is currently not very financially rewarding in the present model of compensation. Maintaining quality and interpreting CCT can be time consuming, and its reimbursement and work RVU is not competitive when compared to other imaging modalities such as echocardiography and SPECT.
Colonel Todd C. Villines, MD, FACC – program director of the cardiology fellowship and director of CCT lab at Walter Reed hospital, as well as a past president of the Society of Cardiovascular Computed Tomography – said that almost all cardiology fellowship graduates at Walter Reed attain level II cardiac training during their fellowship. He believes that "the clinical utilization of cardiac CT is now supported by robust clinical evidence that document significant improvements in health outcomes as compared to usual care. As guidelines and payers increasingly endorse CCT across a broad array of clinical indications, there exists a marked need to train more cardiology fellows to perform and interpret cardiac CT studies. CCT is a skill that can be obtained during general cardiology fellowship, provided that interested fellows have access to a high-volume, high-quality CCT lab and excellent clinician mentors."
The advantages of pursuing level II cardiac CT training are plentiful, and they outweigh the potential disadvantages. General cardiology fellows should be aware of the possibility and benefits of obtaining CCT training within the three-year span of their fellowship. For those interested in running a CCT lab, pursing a research career in CCT, or want to pursue complex cases such as structural heart disease, a full dedicated year to acquire level III CCT training may be more appropriate.
Table 1: Requirements for different training levels CCT1 and Cardiac MR2&3. #
|
Cardiac CT |
Cardiac MR |
Level I |
1-A minimum of supervised interpretation of 50 CCT examinations |
1-A minimum of 4 weeks of cumulative exposure to CMR |
Level II |
1-A minimum of supervised interpretation of 250 CCT examinations |
1-A minimum of 12 weeks of dedicated CMR training |
Level III |
1-Completion of level II |
1-A minimum of 12 months training in CMR |
1 http://www.onlinejacc.org/content/65/17/1810 |
||
Figure 1:
This article was authored by Thura T. Harfi, MD, MPH, assistant professor of internal medicine in the Division of Cardiology, Department of Medicine at the Ohio State University Wexner Medical Center in Columbus, OH.