An 86 year old woman presented to clinic with persistent shortness of breath and lower extremity edema after transcatheter aortic valve replacement (TAVR). She had undergone implantation of a 23-mm Edwards SAPIEN bioprosthetic valve for severe calcific aortic stenosis one month prior to presentation via a transfemoral approach. Clinical evaluation was notable for a blood pressure of 138/67, bilateral pitting lower extremity edema, and a new holodiastolic murmur. The patient was referred for transthoracic echocardiography (Figure 1) and cardiovascular magnetic resonance (CMR) imaging (Figure 2 and Videos 1-3) for further evaluation of suspected paravalvular leak (PVL).
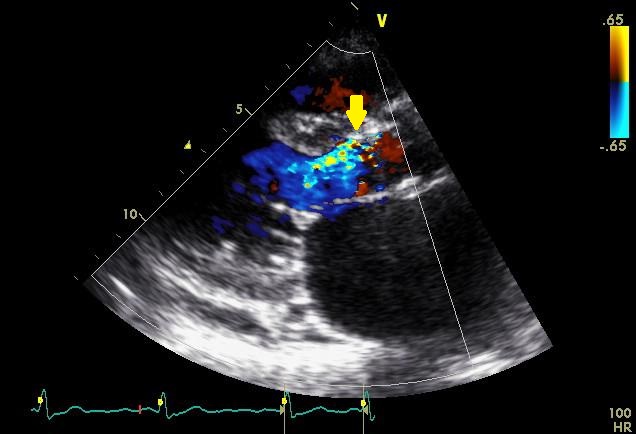
Figure 1
Two-dimensional transthoracic echocardiographic parasternal long axis image demonstrating severe paravalvular leak (arrow).
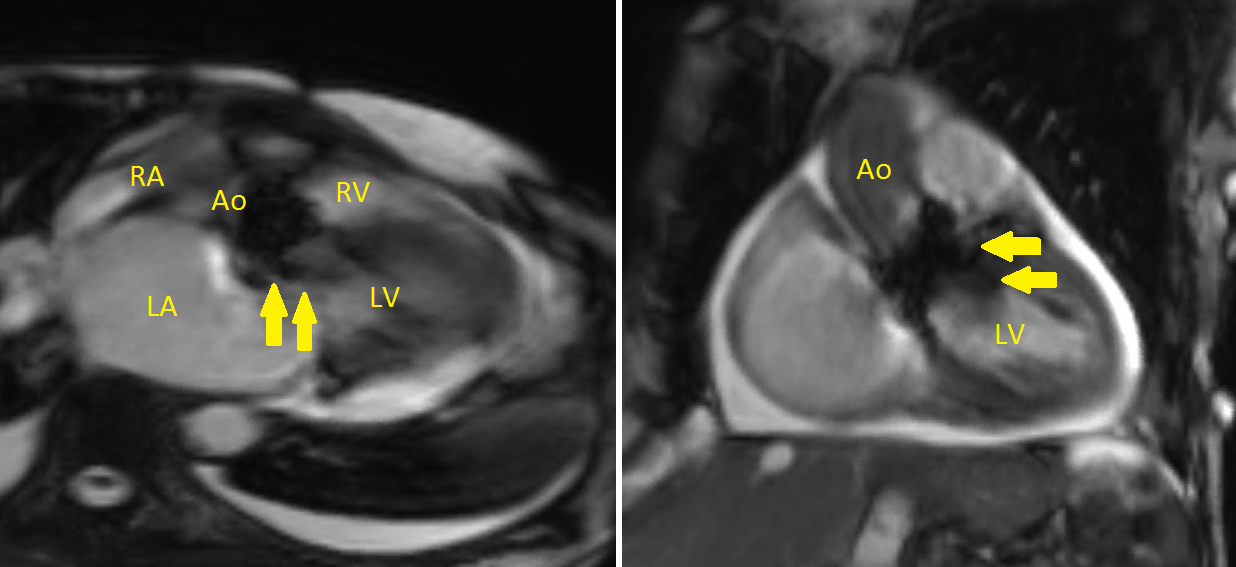
Figure 2
Representative views of the paravalvular regurgitation on cardiac magnetic resonance imaging (arrows). Ao = aorta. LA = left atrium. LV = left ventricle. RA = right atrium. RV = right ventricle.
Video 1
Transverse view of the paravalvular leak on cardiac magnetic resonance imaging. Backflow of blood is seen in the left ventricular outflow tract as the left ventricle relaxes during diastole.
Video 2
Sagittal view of the paravalvular leak on cardiac magnetic resonance imaging.
Video 3
Coronal view of the paravalvular leak on cardiac magnetic resonance imaging.
Which of the following statements about PVL after TAVR is true?
Show Answer
The correct answer is: B. In the PARTNER trial, PVL was associated with an increased risk of mortality.
The echocardiographic and CMR images demonstrate severe paravalvular leak (PVL). Moderate or severe PVL is more common after TAVR than surgical aortic valve replacement (SAVR), with an incidence of approximately 14% for TAVR versus 1% for SAVR at 30 days.1 PVL is an independent predictor of mortality after the procedure, and the mortality risk is proportional to the severity of the regurgitation.1,2 Even mild PVL was associated with an increased risk of mortality post-TAVR in the PARTNER trial,1,2 though most other studies have not reported worse outcomes with mild or trace PVL.3 Approximately 22% of patients have an increase in regurgitation severity by at least one grade at 2 years follow-up.2
Paravalvular regurgitation after TAVR may be related to annular issues (i.e. calcification) or technical and device-related issues (i.e. valve undersizing or maldeployment).3,4 Due to the elliptical nature of the aortic annulus and acoustic shadowing related to significant annular or leaflet calcification, valve sizing remains a challenge. Modalities that have been used to improve the accuracy of annular measurement include cardiac computed tomography and three-dimensional echocardiography.5-7 Oversizing the valve by at least 1 mm relative to the mean annular diameter or by at least 10% relative to the annular area may reduce the risk of significant PVL.6 However, risks of oversizing may include annular rupture, coronary artery occlusion, and arrhythmias.3
The assessment of PVL severity by echocardiography is not straightforward, due to shielding and reverberations from the valvular frame as well as the eccentric nature of the regurgitant jets, with associated crescentic, irregular regurgitant orifices.3,4 Several guidelines regarding the grading of PVL severity have been published; these incorporate the use of semi-quantitative parameters such as jet width (as a percentage of left ventricular outflow tract width) and diastolic flow reversal in the proximal descending aorta, as well as quantitative parameters, such as regurgitant volume, regurgitant fraction, and effective regurgitant orifice area.8-10 One suggested semi-quantitative criterion involves the circumferential extent of PVL expressed as a percentage of the aortic annular circumference on the short-axis view (Figure 3). In this scheme, mild PVL is characterized as involving < 10% of the aortic annular circumference, moderate PVL is characterized as involving 10-29% of the circumference, and severe PVL is characterized as involving ≥ 30% of the circumference.8 However, this diverges from previous publications in which moderate PVL involves 10-20% of the annular circumference and severe PVL involves > 20% of the annular circumference.9-10 The authors do acknowledge that this criterion is not well-validated and may overestimate the severity of PVL compared to quantitative Doppler.8 Recently, cardiovascular magnetic resonance (CMR) imaging has emerged as another option to delineate PVL severity.11 When compared to cardiovascular magnetic resonance (CMR) imaging, echocardiographic circumferential extent may actually tend to overestimate PVL severity.12 Greater than mild PVL by CMR (defined as a regurgitant fraction > 20%) has been associated with a higher incidence of adverse events.13 In our patient, the regurgitant fraction by CMR was calculated to be 42.5% (Figure 4A).
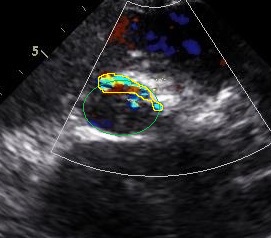
Figure 3
Two-dimensional transthoracic echocardiographic short axis image with superimposed color Doppler demonstrating the circumferential extent of paravalvular leak (yellow tracing). The aortic annulus is outlined in green.
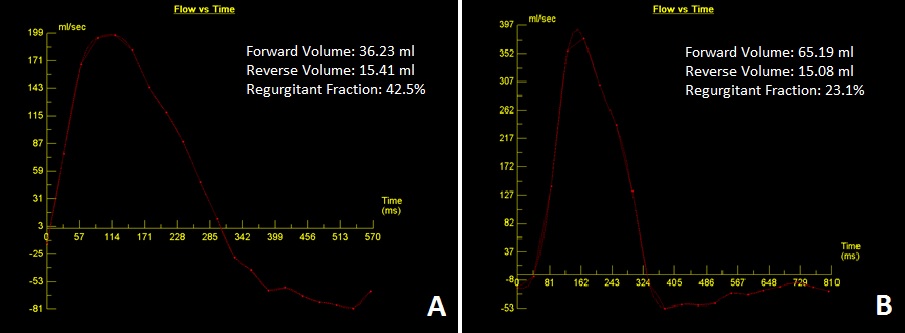
Figure 4A/4B
Velocity versus time curves generated from cardiovascular magnetic resonance phase contrast velocity mapping for flow quantification. Panel A demonstrates the curve obtained prior to referral for transcatheter device closure, with a regurgitant fraction of 42.5%. Panel B demonstrates the curve obtained after transcatheter device closure, with reduction of the regurgitant fraction to 23.1%.
There are no universally established guidelines for management of post-TAVR PVL;3 management is generally individualized and dependent on operator expertise, as well as the acuity or chronicity of the PVL post-TAVR. Management options for acute PVL after immediately after TAVR include post-implantation balloon dilation, valve repositioning by snaring, valve-in-valve replacement, or surgical conversion.3,4,14-16 Post-implantation balloon dilation has been associated with a reduction in PVL severity by at least one grade in 71% of patients.14 In patients with chronic PVL after TAVR, transcatheter device closure is an option.17-18 There are no devices currently available that are specific for transcatheter device closure post-TAVR; off-label use of the Amplatzer Vascular Plug II is the most common device used for this purpose.18 Our patient was referred for transcatheter device closure with this device. The procedure was successful in reducing the regurgitant fraction to 23.1% (Figure 4B). The patient's symptoms improved substantially after the procedure, and she continues to do well at follow-up.
References
Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement of surgical aortic valve replacement for high risk surgical patients with aortic stenosis (PARNTER 1): a randomised controlled trial. Lancet 2015; Epub 15 Mar 2015.
Kodali SK, Williams MR, Smith CR, et al. Two-year outcomes after transcatheter or surgical aortic-valve replacement. N Engl J Med 2012;366:1686-95.
Lerakis S, Hayek SS, Douglas PS. Paravalvular aortic leak after transcatheter aortic valve replacement: current knowledge. Circulation 2013;127:397-407.
Généreux P, Head SJ, Hahn R, et al. Paravalvular leak after transcatheter aortic valve replacement: the new Achilles' heel? A comprehensive review of the literature. J Am Coll Cardiol 2013;61:1125-36.
Jilaihawi H, Kashif M, Fontana G, et al. Cross-sectional computed tomographic assessment improves accuracy of aortic annular sizing for transcatheter aortic valve replacement and reduces the incidence of paravalvular regurgitation. J Am Coll Cardiol 2012;59:1275-86.
Wilson AB, Webb JG, Labounty TM, et al. 3-dimensional aortic annular assessment by multidetector computed tomography predicts moderate or severe paravalvular regurgitation after transcatheter aortic valve replacement: a multicenter retrospective analysis. J Am Coll Cardiol 2012;59:1287-94.
Husser O, Rauch S, Endemann DH, et al. Impact of three-dimensional transesophageal echocardiography on prosthesis sizing for transcatheter aortic valve implantation. Catheter Cardiovasc Interv 2012;80:956-63.
Kappetein AP, Head SJ, Généreux P, et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium-2 consensus document (VARC-2). Eur J Cardiothorac Surg 2012;42:S45-60.
Zoghbi WA, Chambers JB, Dumesnil JG, et al. Recommendations for evaluation of prosthetic valves with echocardiography and Doppler ultrasound. J Am Soc Echocardiogr 2009;22:975-1014.
Zamorano JL, Badano LP, Bruce C, et al. EAE/ASE recommendations for the use of echocardiography in new transcatheter interventions for valvular heart disease. J Am Soc Echocardiogr 2011;24:937-65.
Lerakis S, Hayek S, Arepalli CD, et al. Cardiac magnetic resonance for paravalvular leaks in post-transcatheter aortic valve replacement. Circulation 2014;129:e430-431.
Hayek S, Sawaya F, Oshinski J, et al. Multiparametric assessment of post-transcatheter aortic valve replacement paravalvular regurgitation grading by transthoracic echocardiography and cardiac magnetic resonance. J Clin Exp Cardiolog 2014;5:291.
Hartlage GR, Babaliaros VC, Thourani VH, et al. The role of cardiovascular magnetic resonance in stratifying paravalvular leak severity after transcatheter aortic valve replacement: an observational outcome study. J Cardiovasc Magn Reson 2014;16:93.
Nombela-Franco L, Rodés-Cabau J, DeLarochellière R, et al. Predictive factors, efficacy, and safety of balloon post-dilation after transcatheter aortic valve implantation with a balloon-expandable valve. JACC Cardiovasc Interv 2012;5:499-512.
Vavouranakis M, Vrachatis DA, Toutouzas KP, et al. "Bail out" procedures for malpositioning of aortic valve prosthesis (CoreValve). Int J Cardiol 2010;145:154-5.
Ussia GP, Barbanti M, Ramondo A, et al. The valve-in-valve technique for treatment of aortic bioprosthesis malposition an analysis of incidence and 1-year clinical outcomes from the Italian CoreValve registry. J Am Coll Cardiol 2011;57:1062-8.
Martinez CA, Singh V, O'Neill BP, et al. Management of paravalvular regurgitation after Edwards SAPIEN transcatheter aortic valve replacement: management of paravalvular regurgitation after TAVR. Catheter Cardiovasc Interv 2013;82:300-11.
Reed GW, Tuzcu EM, Kapadia SR, et al. Catheter-based closure of paravalvular leak. Expert Rev Cardiovasc Ther 2014;12:681-692.