To reinforce that heart failure in the presence of a preserved ejection fraction has a diverse set of causes.
To define the underlying etiology, which is essential for appropriate treatment.
To highlight features of an infiltrative cardiomyopathy as a cause of heart failure with preserved ejection fraction (HFpEF) in order to facilitate early diagnosis.
Case Presentation
You are asked to evaluate an 82-years-old woman with exertional dyspnea and near-syncope as a second opinion. According to her son, who accompanied her to the appointment, she has been slowing down for the past year or two. She has had previous evaluations at three different medical centers for these symptoms. She has been treated at each institution with diuretics for acute decompensated heart failure and, because of a positive troponin, has undergone three cardiac catheterizations, none of which demonstrated significant coronary artery disease.
Currently, she can walk about two blocks and one flight of stairs because of dyspnea on exertion compatible with New York Heart Association (NYHA) Class IIB symptoms. She denies paroxysmal nocturnal dyspnea (PND) and orthopnea, although she does have nocturia. She has no bloating or edema. She has learned to eat a low-sodium diet and check her weight daily.
Review of systems: No easy bruising, no history of carpal tunnel syndrome, arthritis affecting her knees and back; bilateral hearing aids; palpitations with activity; no history of hypertension; inflammatory bowel disease, in remission, no melena or bright red blood per rectum.
Physical exam: Amicable elderly woman in no acute distress. She is 5 feet, 3 inches, weighs 157 pounds. Her heart rate was 78 bpm, increased to 100 bpm with a hall walk. Her blood pressure was 124/80; O2 saturation was 96% on room air and stayed at 96% with activity. Her skin was warm. She had JVP at 10 cm with a rapid x and y descent. Her lung fields were clear bilaterally without an audible gallop or murmur. She had crackles at her bases. Her abdomen was soft and non-tender with no organomegaly. She had trace ankle edema
Previous workup available for review includes the following:
An echocardiogram showed a left atrium of 43 mm, septal wall thickness was 13 mm, left ventricular internal dimension in diastole was 42 mm, EF was 73%, her E:A ratio was 0.72 and right ventricular systolic pressure (RVSP) was estimated at 38 mm Hg. She had mild aortic regurgitation (AR), no aortic stenosis (AS), mild mitral regurgitation (MR), mild mitral annular calcification, and trivial pericardial effusion.
A left heart catheterization demonstrated that left ventricular (LV) pressure was 100/12 mm Hg, her aortic pressure was 100/55 mm Hg with a mean of 70 mm Hg. Coronary angiography revealed a right coronary artery lesion of 30% in the mid-portion, the left main was normal, proximal left anterior descending (LAD) artery was 30-50% calcified lesion, proximal left circumflex was mildly diseased and distally had a 30-50% stenosis. She had an EF of 55% on left ventriculogram and 1+ MR.
A right heart catheterization at rest and with exercise was performed two years ago. Her resting right atrial (RA) pressure was 12 mm Hg, RV was 35/12 mm Hg, and pulmonary artery (PA) pressures were 32/12 mm Hg with a mean of 20 mm Hg. Pulmonary capillary wedge pressure was 12 mm Hg. PA saturation was 62%. Her aortic saturation was 92%, resting cardiac output of 5 L/min, cardiac index was 2.8 L/min/m2, and her pulmonary vascular resistance (PVR) was 1.6. With exercise, her blood pressure went to 110/60 with a mean of 77 mm Hg. Her aortic saturation stayed at 93%, her pulmonary artery saturation was 57%, and pulmonary capillary wedge pressure rose to 20 mm hg, PA pressures increased to 55/20 mm Hg with a mean of 32 mm Hg. Her cardiac output fell to 4.4 L/min, her cardiac index was 2.5 L/min/m2, and her PVR was 2.7.
Laboratory testing available for review: Blood urea nitrogen (BUN) of 26, creatinine of 1.2, albumin of 3.5, normal liver function tests (LFTs), an estimated glomerular filtration rate of 42 ml/min/m2. Her total cholesterol was 150, LDL of 80, hemoglobin of 10.9 with a platelet count of 194 and a white count of 8.7.
Laboratory testing today including a troponin that was positive at 0.45 ng/ml (normal <0.02 ng/ml), and her B-type natriuretic peptide (BNP) level was 871 pg/ml (normal <100 pg/ml). Her potassium was 4, sodium was 140, BUN 29, creatinine 1.34. Her glucose was 85.
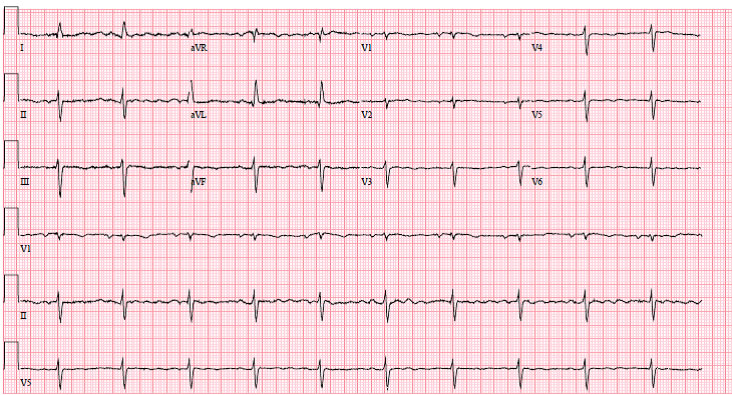
Electrocardiogram (ECG): Sinus rhythm, leftward axis, probable left atrial enlargement, poor R-wave progression, normal voltage (Figure 1).
Figure 1
Which of the following blood tests is most likely to suggest an important, previously unrecognized diagnosis in this patient?
Show Answer
The correct answer is: D. Serum kappa and lambda free light chains.
Explanation: This patient has a heart failure syndrome in the setting of a preserved EF. Interestingly, she has neither history of hypertension, which is prevalent almost 80-90% of individuals with HFpEF,1 nor significant coronary disease, which is prevalent in >60% of subjects with HFpEF.2 The presence of HFpEF in the absence of hypertension should suggest the presence of unusual conditions that limit stroke volume and cardiac output (e.g., infiltrative disorders, hypertrophic cardiomyopathy and pericardial disease).3 An echocardiogram reveals increased wall thickness, which is not accompanied by a concomitant increase in voltage on her 12-lead ECG.
These features coupled with the elevated filling pressure on right heart catheterization, physical exam findings of a rapid x and y descent on assessment of jugular venous pulsation, left atrial size that is greater than left ventricular size along with elevated biomarkers including BNP and troponin are all suggestive of an infiltrative disease, such as amyloid. Accordingly, given the high suspicion for amyloidosis and that light-chain (AL) amyloid is the most malignant type of amyloid, serum kappa and lambda free light chains (which have the highest sensitivity for identifying a plasma cell dyscrasia) are the next best test to order.
Commentary: While an SPEP is a reasonable test to evaluate for a plasma cell dyscrasia, the sensitivity of an SPEP with or without immunofixation is significantly less than that of the light chain assay.4 Assessment of iron stores could raise the possibility of iron overload, although in hemochromatosis patients usually are not anemic (as in this case), patients with anemia and iron overload usually are receiving chronic transfusions, and the clinical presentation of patients with iron overload usually does not involve significant elevation in cardiac biomarkers.5 Elevated angiotensin-converting enzyme levels can be seen in cardiac sarcoidosis,6 but such testing is not recommended for routine screening, and the clinical course of this patient is not typical of cardiac sarcoidosis (e.g., no evidence of conduction disease). Finally, testing for Lyme antibodies would be useful to establish exposure to Borrelia burgdorferi (the etiologic cause of Lyme carditis), but none of the typical features of Lyme disease (e.g., bull’s eye rash, heart block, arthritis) are present.
Epilogue: The patient had a lambda free light-chain level of 18.3 mg/dl (normal 0.33 to 1.94 mg/dl) with a normal kappa free light chain of 1.9 (normal 0.57 to 2.63) and an altered ratio of 9.6 (normal 0.26 to 1.65). SPEP and immunofixation electrophoresis demonstrated the continuous presence a monoclonal IgA lambda in the gamma region at a concentration of 0.6 g/dl. A right heart catheterization demonstrated a right atrial pressure of 11 mm Hg, right ventricluar pressure of 43 /11 mm Hg, pulmonary artery pressure of 41/20 (27) mm Hg, pulmonary wedge pressure of 17 mm Hg with a pulmonary artery saturation of 58% and an aortic saturation of 96%, with a cardiac output of 2.97 l/min and cardiac index of 1.74 l/min/m by the Fick equation. An endomyocardial biopsy demonstrated endocardial infiltration with a homogeneous amorphous pink material. The congo red, crystal violet, and trichrome stains confirmed the material as amyloid. There was also focal interstitial involvement and vascular involvement, favoring primary (AL) amyloid over senile (transthyretin-related amyloidosis [ATTR]) amyoid. The trichrome stain also showed mild endocardial and interstitial fibrosis. No iron was demonstrated with the iron stain. Liquid chromatography tandem mass spectrometry was performed on peptides extracted from Congo red-positive areas and detected a peptide profile consistent with AL (lambda)-type amyloid deposition. A bone marrow biopsy confirmed the presence of lambda restricted plasma cells (~10%). She had no evidence of multiple myeloma. She was started on targeted plasma cell therapy with Cytoxan, Bortezomib and Dexamethasone (CyBorgD).7
References:
Mohammed SF, Borlaug BA, Roger VL, et al. Comorbidity and ventricular and vascular structure and function in heart failure with preserved ejection fraction: a community-based study. Circ Heart Fail 2012;5:710-9.
Hwang SJ, Melenovsky V, Borlaug BA. Implications of coronary artery disease in heart failure with preserved ejection fraction. J Am Coll Cardiol. 2014;63:2817-27.
Kliger C, King DL, Maurer MS. A clinical algorithm to differentiate heart failure with a normal ejection fraction by pathophysiologic mechanism. Am J Geriatr Cardiol 2006;15:50-7.
Palladini G, Russo P, Bosoni T, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine. Clin Chem 2009;55:499-504.
Tanner MA, Galanello R, Dessi C, et al. Myocardial iron loading in patients with thalassemia major on deferoxamine chelation. J Cardiovasc Magn Reson 2006;8:543-7.
Lieberman J. Elevation of serum angiotensin-converting-enzyme (ACE) level in sarcoidosis. Am J Med 1975;59:365-72.
Venner CP, Lane T, Foard D, et al. Cyclophosphamide, bortezomib, and dexamethasone therapy in AL amyloidosis is associated with high clonal response rates and prolonged progression-free survival. Blood 2012;119:4387-90.