A 22-year-old man who was otherwise healthy presented to the emergency department with 2 days of worsening left-sided pleuritic chest pain and one episode of hemoptysis. The patient's physical examination revealed a diastolic murmur at the apex. The electrocardiogram and chest X-ray were unremarkable. In the emergency department, computed tomography angiography (CTA) of the chest was performed to assess for pulmonary embolism (Figure 1). Based on CTA findings, subsequent transthoracic echocardiogram (TTE) and transesophageal echocardiogram (TEE) were obtained (Videos 1-3).
Figure 1
Video 1
Video 2
Video 3
What do you think this mass is?
Show Answer
The correct answer is: D. Malignant cardiac tumor
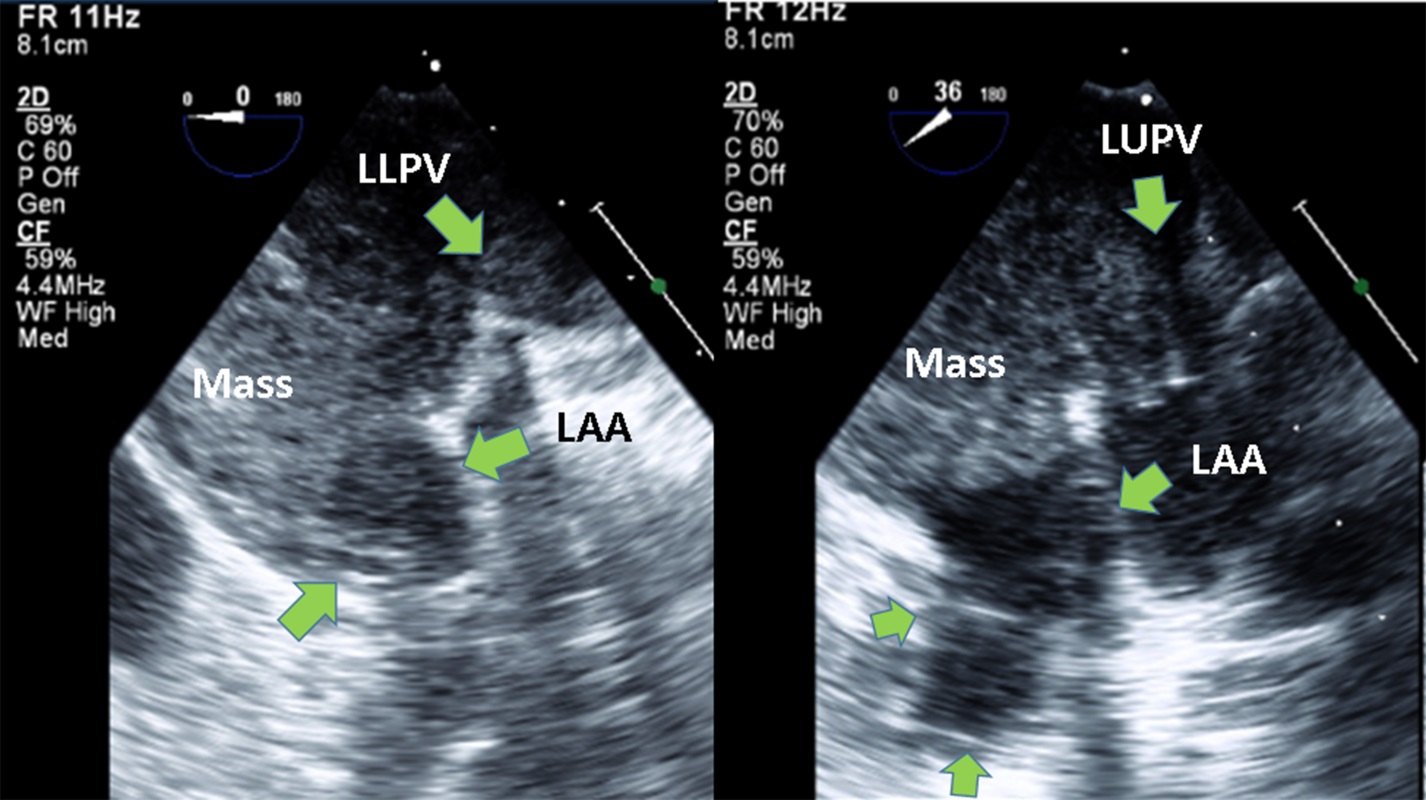
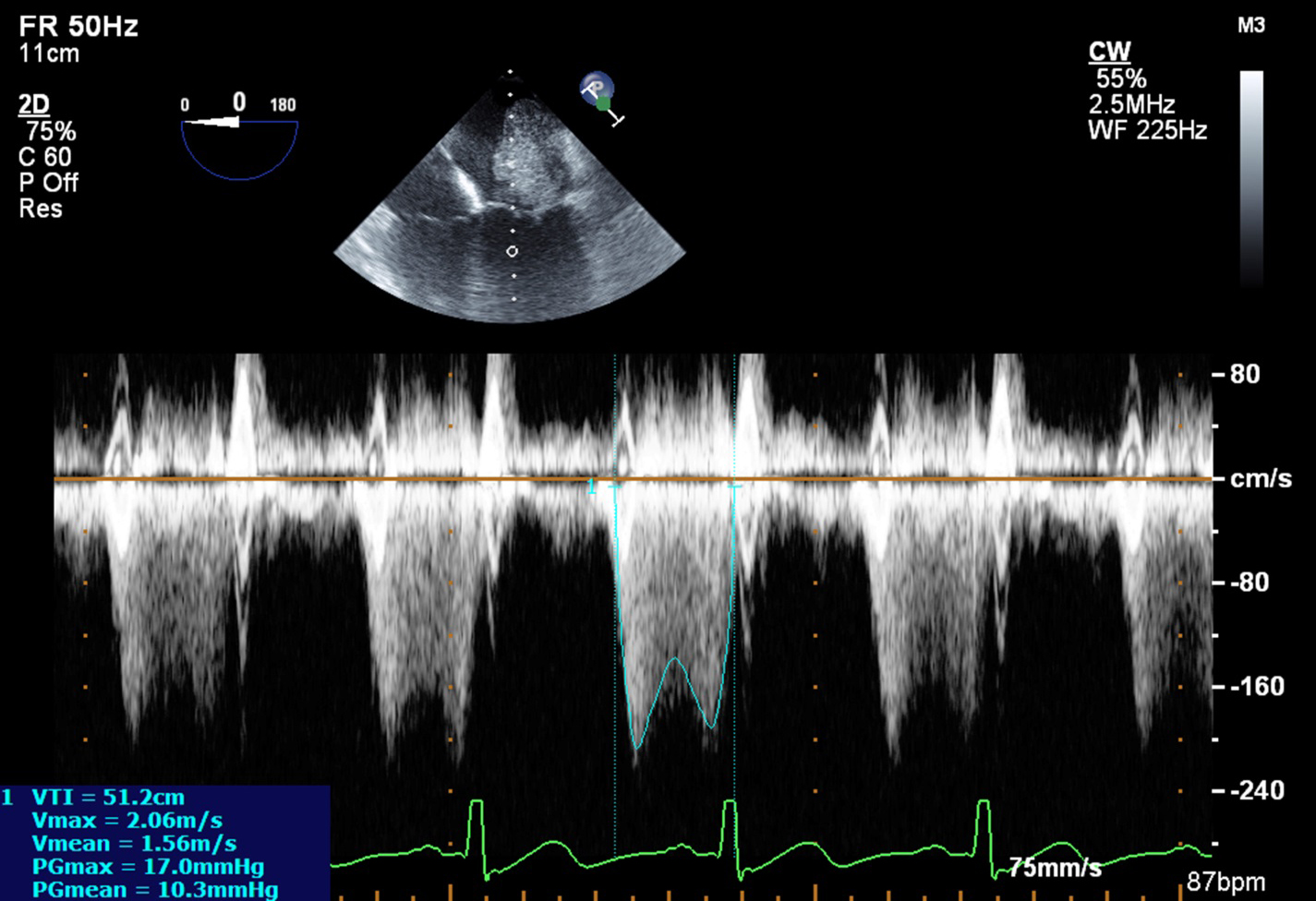
The CTA of the chest showed a 4.2 x 5.1 cm left atrial (LA) mass (Figure 1, green arrow) completely obstructing the left inferior pulmonary vein and partially obstructing the left upper pulmonary vein (Figure 1, red arrow). The TTE and TEE confirmed a large LA mass that involved the appendage as well as both left pulmonary veins (Videos 1-3 and Figure 2). It was associated with obstruction of mitral inflow with moderate-to-severe mitral stenosis with peak/mean gradient = 17/10 mm Hg (heart rate = 87 bpm) (Figure 3). As assessed by contrast echocardiography, the mass was not highly vascular.
Figure 2
Figure 3
Atrial Myxoma
This benign tumor is the most common cardiac neoplasm, accounting for more than 75% of primary cardiac tumors. It typically originates from the left side of the fossa ovalis but can be seen in the right atrium in about 20% of case and elsewhere in a smaller number of cases. A number of features have been proposed to differentiate between myxoma and sarcoma, with the following features being highly suggestive of a sarcoma:
Nonseptal origin
Broad attachment on the LA wall
Extension to or from the pulmonary veins
Semisolid consistency
Multiple masses1
The first four features can be recognized in this patient. The key finding that points to this being a malignant tumor is the involvement of the pulmonary veins. Indeed, an intra-atrial mass that involves any of these veins should be presumed to be malignant. Although echo contrast enhancement can be seen in malignant tumors, absence of contrast enhancement does not exclude a malignant process.
Mitral Vegetation
Because the mass was not attached to the mitral leaflets and there were no systemic symptoms or signs to support the diagnosis of endocarditis, vegetation can be excluded.
Cardiac Thrombus
Cardiac thrombi are the most common LA masses; however, they are rarely seen on TTE. They are typically associated with spontaneous echo contrast and usually involve the LA appendage. This patient lacks typical risk factors predisposing to stasis and thrombus formation such as rheumatic valve disease, atrial fibrillation, and left ventricular systolic dysfunction. Although involvement of the appendage is typical of thrombus, involvement of the pulmonary veins is not.
Clinical Course
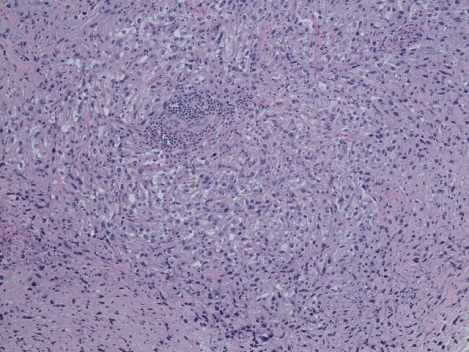
A complete surgical resection was attempted in this patient, but a small rim of tumor deep in the left inferior pulmonary vein was inaccessible and left behind. Surgical pathology and immunologic staining were consistent with an intimal type primary sarcoma (Figure 4).
Figure 4
Discussion
Primary sarcomas of the heart and great vessels are rare clinical entities. Their presentation depends primarily on their location rather than their histologic types. LA masses can present with symptoms of pulmonary hypertension as dyspnea and hemoptysis, as in this patient. Less common presentations may include embolization of tumor fragments or superimposed thrombus to the systemic or pulmonary circulation and arrhythmias related to tumor infiltration into the myocardium.
Treatment of primary cardiac sarcomas represents a unique challenge because of their high rate of recurrence after excision and their tendency to metastasize early. In the largest series of treated cases of primary cardiac or great vessel sarcomas involving 34 patients over a 32-year period, mean survival was 12 months.2 Data on adjuvant chemotherapy are scarce, and this treatment does not appear to significantly alter the prognosis.
Although not done in this case, cardiac magnetic resonance imaging may also be used to further define the location and composition of intracardiac masses. Signal intensity in sarcomas is typically variable; in myxomas, it is low on T1- weighted images and high on T2-weighted images, owing to abundant polysaccharide-rich ground substance.3
References
Mich RJ, Gillam LD, Weyman AE. Osteogenic sarcomas mimicking left atrial myxomas: clinical and two-dimensional echocardiographic features. J Am Coll Cardiol 1985;6:1422-7.
Simpson L, Kumar SK, Okuno SH, et al. Malignant primary cardiac tumors: review of a single institution experience. Cancer 2008;112:2440-6.
Grebenc ML, Rosado de Christenson ML, Burke AP, Green CE, Galvin JR. Primary cardiac and pericardial neoplasms: radiologic-pathologic correlation. Radiographics 2000;20:1073-103;1110-12.