Constrictive Pericarditis Following Heart Transplant
Feb 29, 2016
|
Font Size
A
A
A
A 60-year-old woman presents with exertional shortness of breath, abdominal distention, lower extremity edema and weight gain. She had a heart transplant 14 years prior for familial hypertrophic cardiomyopathy. Over the last few years she has experienced recurrent episodes of volume overload which have been treated with diuretics by her local doctor. Otherwise, she has had an unremarkable post-transplant course, including no history of rejection on surveillance endomyocardial biopsies. Home medications include tacrolimus, mycophenolate mofetil, rosuvastatin, aspirin, lisinopril, and furosemide. Physical exam is notable for jugular venous distention to the angle of the jaw when the patient is upright at 90 degrees with a rapid y descent, distended abdomen with fluid wave, and 3+ pitting lower extremity edema to the mid-thigh. Selected clips from a transthoracic echocardiogram (TTE) and cardiac magnetic resonance imaging (MRI) are displayed in Videos 1-5.
Cardiac catheterization demonstrates the following measurements with select hemodynamic tracings shown in Figures 1 and 2.
RA = 23 mmHg
RV = 42/23 mmHg
PA = 32/23 mmHg, mean = 30 mmHg
PCWP = 23 mmHg
LV = 120/23 mmHg
Cardiac output = 7.85 L/min
The patient is diagnosed with constrictive pericarditis and referred for further management.
Video 1
Video 1: TTE, parasternal long axis view demonstrating dilated left atrium and pericardial thickening of the posterior wall
Video 2
Video 2: TTE, parasternal short axis view demonstrating leftward shift of the interventricular septum during inspiration
Video 3
Video 3: TTE, apical four chamber view demonstrating ventricular septal bounce and conical compression of the right ventricle
Video 4
Video 4: Cardiac MRI demonstrating restricted right ventricular movement and diastolic septal bounce
Video 5
Video 5: Cardiac MRI demonstrating respirophasic shift with ventricular interdependence
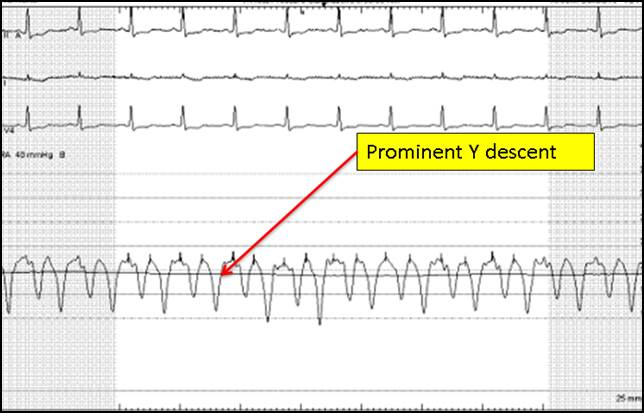
Figure 1
Figure 1: Right atrial waveform demonstrating prominent Y descent
Figure 2
Figure 2: Right ventricular waveform demonstrating a diastolic dip and plateau tracing, also called the "square root" sign
Which of the following statements is true regarding surgical pericardiectomy for constrictive pericarditis?
Show Answer
The correct answer is: C. Constrictive pericarditis following heart transplant is rare and there is little evidence to guide management
Pericardiectomy can be an effective treatment for patients with symptomatic constrictive pericarditis. However, outcomes after pericardiectomy are closely associated with underlying etiology, left ventricular systolic function, and other co-morbidities. The most common etiology of constrictive pericarditis requiring pericardiectomy is idiopathic, followed by postsurgical and postradiation. Studies indicate that overall perioperative mortality ranges from 5-6%. Patients with idiopathic constrictive pericarditis typically have the best outcomes following pericardiectomy, and postradiation is a strong predictor of poor outcome (>20% perioperative mortality). No studies have established a clear benefit for any particular surgical approach with regard to perioperative mortality or long-term survival.
Constrictive pericarditis following cardiac transplantation is rare and data are limited to case reports and small case series. Pericardial injury, irritation, bleeding, and infection predispose to postoperative pericardial fibrosis and constriction. Pericardiectomy is generally the treatment of choice; however, chronic cardiac rejection may present with similar hemodynamic findings, in which case pericardiectomy has been associated with poor outcomes. Overall, data are limited to guide therapy and treatment should be determined on a case by case basis.
References
Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis: etiology and cause-specific survival after pericardiectomy. J Am Coll Cardiol. Apr 21 2004;43(8):1445-1452.
Bansal R, Perez L, Razzouk A, Wang N, Bailey L. Pericardial constriction after cardiac transplantation. J Heart Lung Transplant. Mar 2010;29(3):371-377.
Hinkamp TJ, Sullivan HJ, Montoya A, Park S, Bartlett L, Pifarre R. Chronic cardiac rejection masking as constrictive pericarditis. Ann Thorac Surg. Jun 1994;57(6):1579-1583.