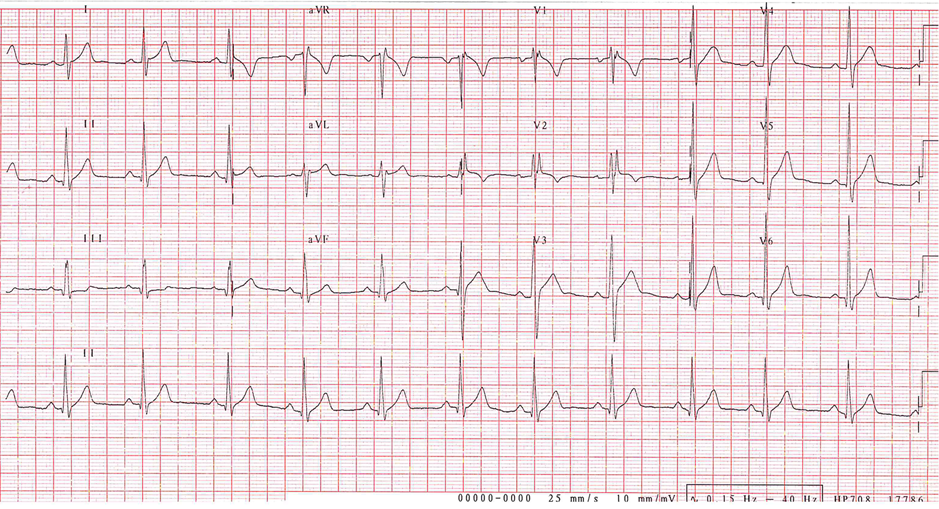
A 19-year-old male collegiate baseball player reports an episode of near syncope while lifting weights. After performing several repetitions while bench pressing, he began to experience lightheadedness and decreased vision. He stopped exercising and after several seconds his symptoms began to resolve. He reports no loss of consciousness, no chest pain, no palpitations, and no shortness of breath. He has not had any similar prior episodes, Otherwise, has exercised without symptoms, and has no difficulty keeping pace with his teammates in both practice and in competition. There is no family history of sudden, early, or unexplained death. Physical examination is grossly normal. Electrocardiogram, shown in Figure 1, was concerning for the question of an epsilon wave in lead V1. A Holter monitor was placed which was grossly normal. Echocardiogram revealed normal right ventricular systolic pressure. Cardiac magnetic resonance imaging (MRI) was performed and is shown in Video 1.
Figure 1
Video 1
At this point, which of the following describes the next best step in management?
Show Answer
The correct answer is: E. Both B and D are correct.
The cardiac MRI illustrated an enlarged right ventricle without fibrofatty infiltration, microaneursyms, or focal hypokinesis. There was a secundum atrial septal defect (ASD) with a QP/QS ratio of 1.9, which likely explained the dilated right heart chambers. No anomalous pulmonary venous connections were noted. Based on the recommendation from the 35th Bethesda Conference that athletes with an ASD and normal pulmonary artery pressures can participate in all competitive sports, our baseball player continued to play through the remainder of the season. However, due to the dilated right heart chambers, the decision was made to close the defect percutaneously in the off-season. Prior to his procedure, he underwent a transesophageal echocardiogram (TEE) with three-dimensional (3-D) imaging to ensure appropriate rims around the defect. 3-D TEE measured the defect area to be 1.5 cm. The ASD measured 1.6 cm anterior-posterior by 0.8 cm superior-inferior on MRI. A right heart catheterization was not performed. He did well having the percutaneous closure in the off-season and subsequently returned to play without incident.
References
Graham TP Jr, Driscoll DJ, Gersony WM, Newburger JW, Rocchini A, Towbin JA. Task Force 2: congenital heart disease. J Am Coll Cardiol 2005;45:1326-1333.
Warnes CA, Williams RG, Bashore TM, et al. ACC/AHA 2008 guidelines for the management of adults with congenital heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines on the Management of Adults With Congenital Heart Disease). Developed in Collaboration With the American Society of Echocardiography, Heart Rhythm Society, International Society for Adult Congenital Heart Disease, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;52:e173-263.