The patient is a 70-year-old male with a history of diabetes mellitus type I, hypertension, hyperlipidemia, anemia, paroxysmal atrial fibrillation, and s/p atrial flutter ablation 6 months ago. He presents with dyspnea on exertion, pedal edema, and weight gain.
An electrocardiogram (ECG) (Figure 1) is performed.
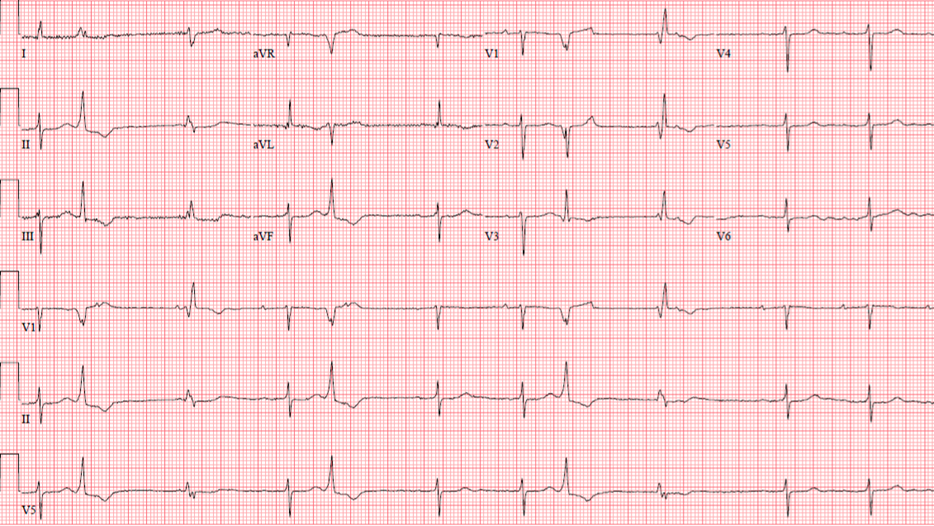
Figure 1
Figure 1
The ECG shows which of the following?
Show Answer
The correct answer is: C. Concealed conduction in the atrioventricular (AV) node
The ECG shows sinus rhythm with prolonged PR, occasional premature ventricular complexes (PVCs) (beats # 2, 5 and 8) as well as junctional escape beats (JEB) with right bundle branch block (RBBB) configuration or ventricular escape beats. Sinus rate is around 63 beat per minutes. The P waves that follow the PVCs are sinus and do not conduct to the ventricle because of the concealed conduction. The QRS axis is leftward with narrow QRS complexes except for junctional beats showing RBBB configuration (beats # 3 and 9). There is no anterior ischemia since T wave changes are related PVCs and RBBB aberration. There is no atrial flutter wave.
Concealed conduction is an electrophysiological phenomenon that occurs when an electrical stimulation conduction does not manifest on ECG. Therefore, it is labelled as concealed conduction. However, it usually has an impact on the next conducted beat.1,2
Concealed conduction is commonly seen with PVCs, which conducts retrogradely to the AV node without further conduction. This will increase the AV node refractoriness which impacts the next beat depending on PVC-P interval:
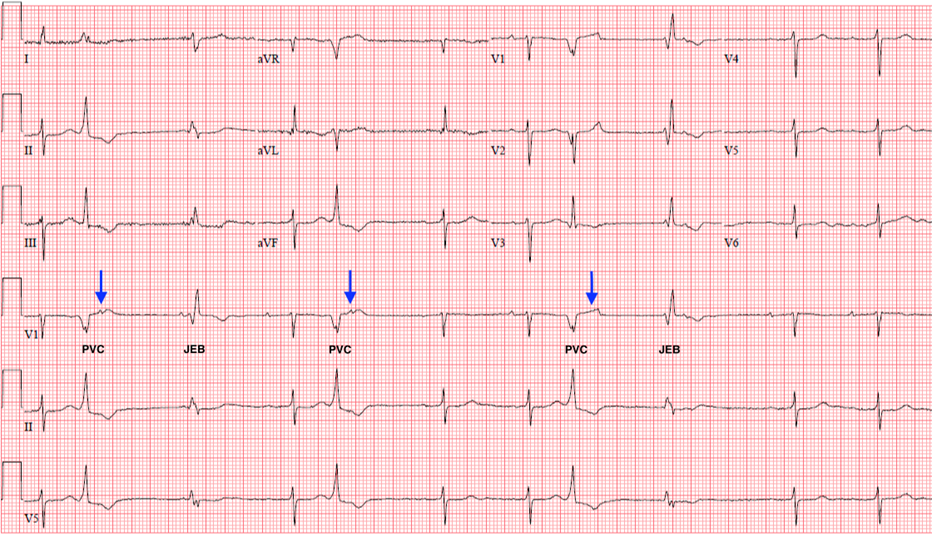
Short PVC-P interval results in AV block (Figure 2, blue arrows) since AV node still in absolute refractoriness. P wave is commonly seen at the early aspect of T wave.
Long PVC-P interval results in prolonged PR if AV node partially recovers and conducts. P wave is commonly seen at the end of T wave or after T wave.1
Figure 2
Figure 2
References
Oh YZ, Tan VH, Wong KCK. Concealed conduction of premature ventricular complexes resulting in AV nodal block. J Arrhythm 2017;33:528-29.
Ari H, Ari S, Koca V, Bozat T. Misleading ECG appearance of AV block due to concealed AV nodal conduction caused by interpolated ventricular ectopic beats. Turk Kardiyol Dern Ars 2009;37:197-200.