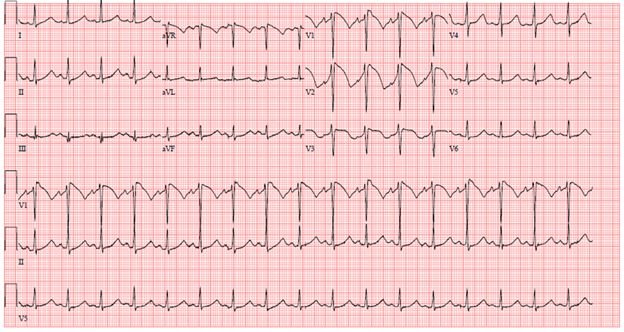
A 50-year-old male with a history of end-stage renal disease and hypertension complained of high-grade temperature, nausea, abdominal pain, and vomiting. He developed sudden onset of palpitation, chest pain and lightheadedness during routine session of dialysis. His heart rate was 110 bpm and temperature of 102 F. He was in the process of being transported to the hospital when he was noted to have polymorphic ventricular tachycardia associated with a brief loss of consciousness. His rhythm returned to sinus rhythm, and he regained consciousness before any resuscitative efforts could be made. The following electrocardiogram (ECG) (Figure 1) was performed at outside hospital emergency department (ED).
Figure 1
Figure 1
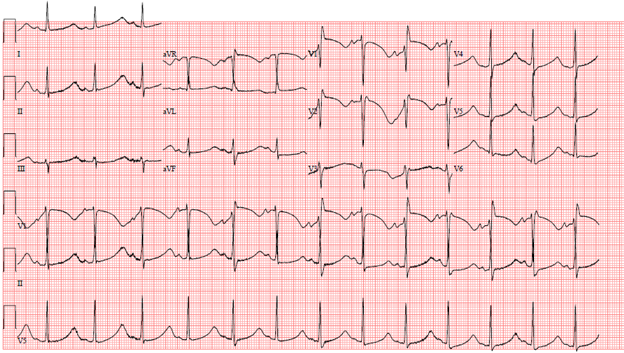
Patient was transferred via emergency squad to our hospital. Intravenous amiodarone drip was initiated in route. He arrived at our hospital ED in stable condition without fever. The following ECG (Figure 2) was performed.
Figure 2
Figure 2
What is the correct diagnosis based on ECG Figures 1 and 2?
Show Answer
The correct answer is: C. Type I Brugada syndrome and QT prolongation
The ST-segment elevations in ECG Figure 1 are classic for type I Brugada pattern ECG. It is characterized by coved-type ST-segment elevation of at least 2 mm followed a descending negative T-wave in at least one right precordial lead (V1 to V3). Patients affected by the disorder can have syncope, seizures, or nocturnal agonal breathing, the latter of which is believed to be secondary to polymorphic ventricular tachycardia or ventricular fibrillation. Fever, as seen in this patient, is often a trigger in those affected.1 It is commonly diagnosed in southeast Asian males.
Of note, the patient initially underwent cardiac catheterization given the ST-elevations and concern for acute coronary syndrome but was found to have non-obstructive coronary artery disease.
In ECG Figure 2, corrected QT interval (QTc) was measured at approximately 750 msec. This prompted cessation of amiodarone given that is a class III antiarrhythmic drug known to prolong cardiac repolarization (QT interval). Importantly, this ECG also demonstrates macrovolt T-wave alternans, a beat-to-beat variation in T-wave amplitude. This ominous sign can often herald malignant ventricular arrhythmias.2
The patient was believed to have a Brugada and prolonged QT overlap syndrome. This phenotype can be caused in certain SCN5A mutations resulting in both gain- and loss-of-function at separate phases of the action potential.3 Ultimately, this patient underwent placement of an implantable cardioverter-defibrillator, was advised to use one pharmacy and avoid drugs that prolong QT interval (https://www.crediblemeds.org was recommended for reference), and was given a referral for genetics counseling.
References
Brugada J, Campuzano O, Arbelo E, Sarquella-Brugada G, Brugada R. Present status of Brugada Syndrome : JACC State-of-the-Art Review. J Am Coll Cardiol 2018;72:1046-59.
Holley CL, Cooper JA. Macrovolt T-wave alternans and polymorphic ventricular tachycardia. Circulation 2009;120:445-46.
Wilde AAM, Amin AS. Clinical spectrum of SCN5A mutations: long QT syndrome, Brugada syndrome, and cardiomyopathy. JACC Clin Electrophysiol 2018;4:569-79.