A 94-year-old veteran with a past medical history of coronary artery disease, hypothyroidism, hypertension, and hyperlipidemia presents to the emergency room complaining of sudden onset pain, numbness, and cramping in his right lower extremity (RLE).
The patient reports that he had a "charley horse" cramping in his entire RLE starting a few hours ago while he was gardening. He states that the pain subsides marginally when he sits down but is still present at rest. The veteran is able to move both lower extremities but complains of a "pins and needles" sensation on the right side. He denies any injury or trauma to that area and has no history of claudication symptoms. The patient is a 55 pack-year smoker but quit 5 years ago. He denies alcohol and illicit drug use.
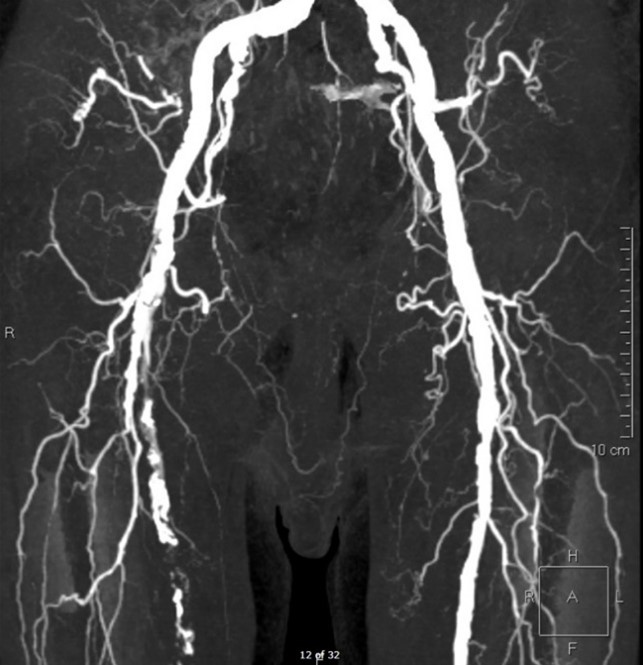
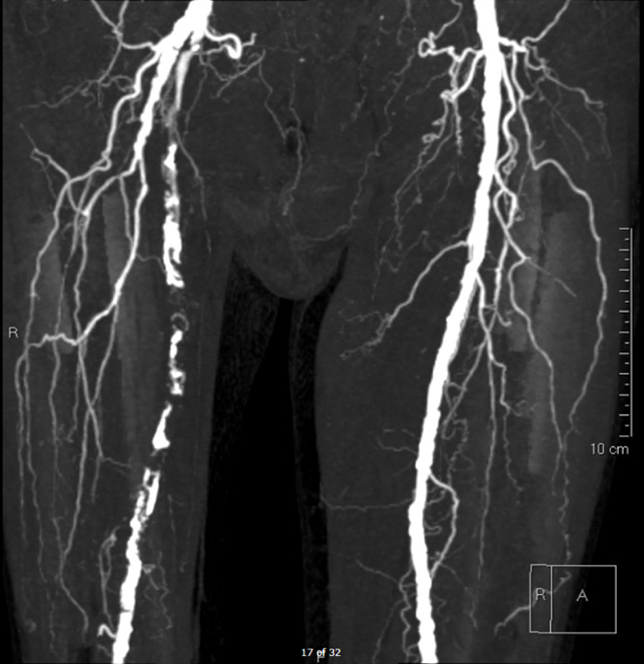
Physical exam of the RLE reveals palpable femoral pulse, but no pulses distally. The patient has decreased sensation and motor strength in the right knee and ankle. His right foot has significant pallor. Examination of the left lower extremity is unremarkable. Bedside ultrasound demonstrates a thrombus in the right common femoral artery. He had monophasic dorsalis pedis signals on the right. Ankle brachial index was 0.4 on the right and 1.06 on the left. Computed tomography angiography (CTA) of the abdomen, pelvis, and bilateral lower extremities was performed, and the images are demonstrated below in Figures 1-4.
Figures 1-4: CTA Images of the Abdomen/Pelvis with Runoff
The correct answer is: D. Emergent revascularization via endovascular treatment, catheter-directed thrombolysis, or open surgical revascularization
Based on the clinical history and CTA findings, this patient's symptoms are most consistent with acute limb ischemia (ALI). ALI is defined as severe limb hypoperfusion of less than 2 weeks duration. Characteristics of ALI are often grouped into the six P's mnemonic: pain, pallor, pulselessness, poikilothermia, paresthesias, and paralaysis.1,2 Typically, neurosensory deficits present earlier than muscle weakness because sensory nerves are affected before motor nerves.3 There are several causes of ALI including embolism, thrombosis, venous obstruction, and trauma.
When ALI is caused by an embolus, the most common source is the heart, but proximal atherosclerotic debris are also common.3 Emboli tend to obstruct arteries at bifurcations where the lumen of the arteries is narrowed. ALI from embolus is usually acutely critical because it typically occurs in a healthy artery where there has been no time to form collateral circulation.
ALI is defined based on the severity of ischemia and is classified as either viable (I), threatened (II), and irreversible (III).1,4 A threatened limb is further broken down into marginally threatened (IIa) and immediately threatened (IIb). These classifications help guide both prognosis and timing or intervention. All patients with ALI should be therapeutically anticoagulated with heparin if there are no contraindications.1,3,5 Heparin does not lyse the clot, but does help preserve the microcirculation by stopping thrombus propagation. In addition to anticoagulation, patients should receive appropriate hydration which may help attenuate the contrast load from angiography and potential myoglobinuria from reperfusion.5
This patient's symptoms most closely align with an immediately threatened Category IIb ALI. The CTA images demonstrate occlusive thrombus involving the majority of the right superficial femoral artery extending from the branch of the profunda femoral artery through the distal superficial femoral artery segment. He has paresthesias with rest pain as well as mild to moderate muscle weakness. In addition to systemic therapeutic anticoagulation with heparin and adequate hydration, patients with a marginally or immediately threatened limb (IIA or IIb) should be treated with emergent endovascular revascularization, catheter-directed thrombolysis, or open surgical revascularization.1,3,5
(Answer A - Conservative therapy with aspirin, statin, cilostazol, and structured exercise program)
This is the appropriate first line treatment for patients with claudication. Unlike the six Ps of ALI, patients with claudication typically present with fatigue, discomfort, cramping, or pain when the affected muscles groups are exerted.1 This commonly presents as lower extremity pain when walking but relieved at rest. The three main goals for treating patients with claudication are to reduce cardiovascular outcomes, increase functional capacity, and prevent limb ischemia.6 In addition to controlling risk factors (smoking cessation, tight glycemic control, statin therapy and strict blood pressure management), first line treatment for claudication includes antiplatelet therapy, statin, cilostazol, and structured exercise therapy.1,7
(Answer B - Admit the patient for overnight observation, adequate analgesia, and hydration)
The acuity in ALI is due to the sudden cessation of oxygen and nutrients to the metabolically active tissues in the limb.2 The goal of revascularization is to prevent limb amputation, so in patients with ALI, time to reperfusion is key prognosticator in determining if the limb can be salvaged.2,3 It would be inappropriate to simply observe a patient with ALI. At minimum, a patient should be anticoagulated to prevent thrombus propagation as long as there are no contraindications.
(Answer C - Schedule urgent endovascular or open surgical revascularization)
Urgent revascularization would be appropriate for patients with Category I ALI.3,5 Patients with Category I ALI have viable limbs without the immediate threat of permanent tissue loss. Patients do not have sensory or motor impairment. They have an audible arterial and venous doppler ultrasound. These patients should be started on anticoagulation and have adequate hydration. They can undergo urgent vascular intervention when their risk factors are optimized.3
(Answer E - Primary amputation)
Amputation would be appropriate for patients with Category III ALI.3,5 Patient's with Type III ALI have non-viable limbs due to prolonged ischemia and permanent nerve damage. These patients have complete loss of sensory and motor function of their limb. They also have an inaudible arterial and venous Doppler ultrasound. Amputation should be the index procedure as the risks associated with attempted revascularization outweigh the benefits in a limb that is non-viable.1,3,5 Reperfusion can lead to multiorgan failure and death due to recirculation of ischemic metabolites.1
References
- Gerhard-Herman MD, Gornik HL, Barrett C, et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2017;69:1465-1508.
- Creager MA, Kaufman JA, Conte MS. Clinical practice. Acute limb ischemia. N Engl J Med 2012;366:2198-2206.
- McNally MM, Univers J. Acute limb ischemia. Surg Clin North Am 2018;98:81-1096.
- Rutherford RB, Baker JD, Ernst C, et al. Recommended standards for reports dealing with lower extremity ischemia: revised version. J Vasc Surg 1997;26:517-38.
- Fluck F, Augustin AM, Bley T, Kickuth R. Current treatment options in acute limb ischemia. Rofo 2020;192:319-26.
- Kullo IJ, Rooke TW. Clinical Practice. Peripheral artery disease. N Engl J Med 2016;374:861-71.
- Kithcart AP, Beckman JA. ACC/AHA versus ESC guidelines for diagnosis and management of peripheral artery disease: JACC Guideline Comparison. J Am Coll Cardiol 2018;72:2789-2801.