A 58-year-old man with a history of atrial fibrillation presents for a routine clinic visit. The patient is on amiodarone and has a history of end-stage renal disease status post renal transplant (2011), gastric neuroendocrine tumor, squamous cell cancer status post Mohs surgery, coronary artery disease, cryptogenic cirrhosis, bioprosthetic aortic valve replacement, and hypothyroidism who took metolazone dose in addition to his usual twice daily torsemide for worsening of pedal edema.
The following ECG is performed:
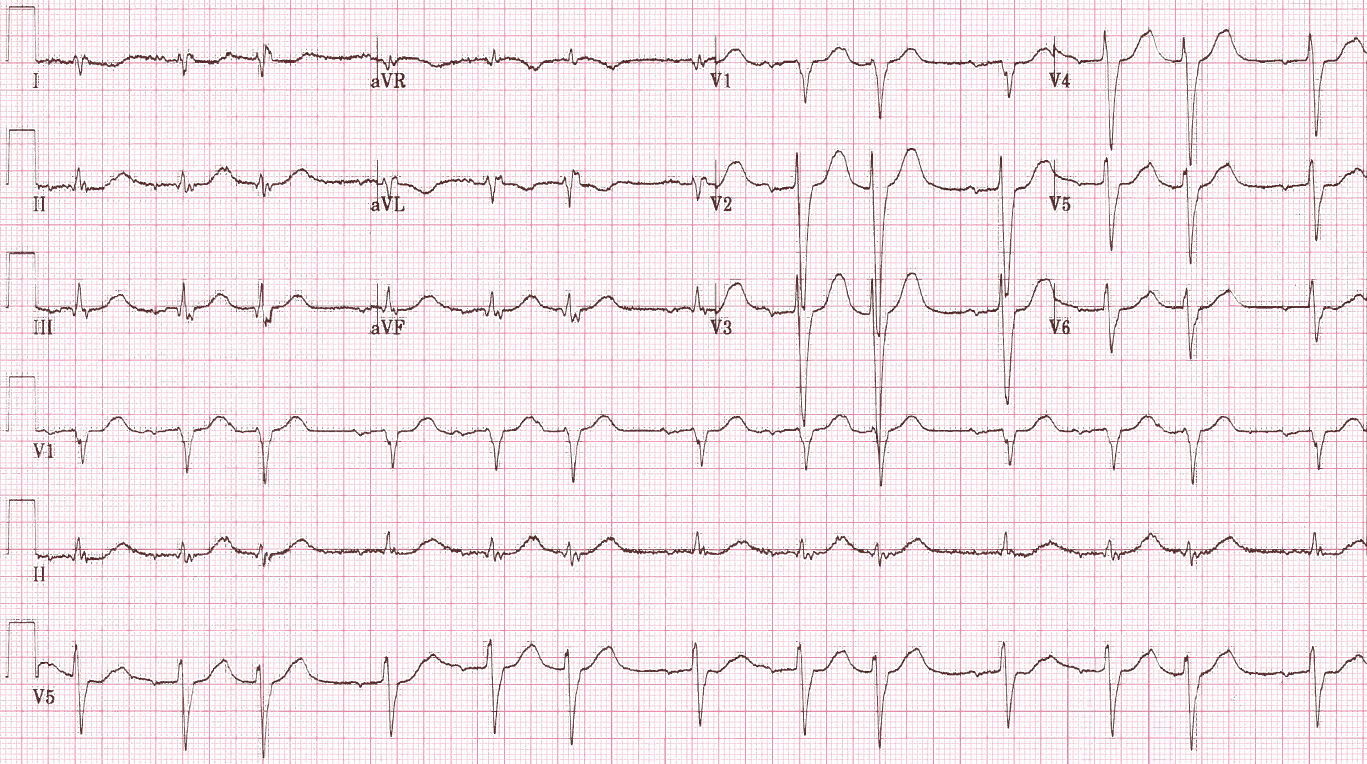
Figure 1
The ECG shows which of the following?
Show Answer
The correct answer is: D. Normal sinus rhythm with premature atrial contraction.
The ECG shows grouped beating in a regularly irregular pattern.
This excludes the possibility of atrial fibrillation. Whenever grouped beating is noted, one must consider the possibility of second-degree AV block (Mobitz I [i.e., AV Wenckebach] or Mobitz II). Wenckebach phenomenon is characterized by progressive prolongation of the conduction time across the AV node (represented by PR interval on the surface ECG), culminating in a dropped beat. This is followed by resumption of Wenckebach periodicity. With Mobitz I or Mobitz II, the P wave rate is nearly constant, given the level of block is intranodal or infranodal, respectively.
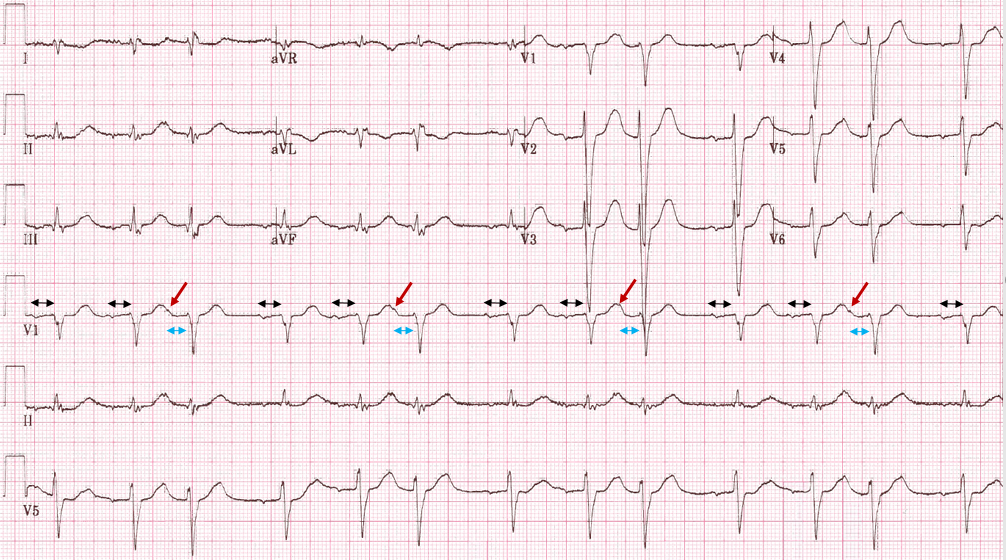
In this ECG, the P wave rate is not constant. The P wave that precedes the longer RR interval comes early. The P wave of the premature atrial contraction is noted at the peak of the T wave of 2nd, 5th, 8th, and 11th beats (red arrows). The PR interval of the 1st and 2nd beats are the same at 240 ms (black arrows). The PR interval of the 3rd beat is shorter at 210 ms (light blue arrows).
Figure 2
The patient was noted to have severe hypokalemia with potassium of 2.7mmol/L. The APDs occurring in a trigeminal pattern resolved with correction of hypokalemia.
References
Zipes DP, Fisch C. Premature atrial contraction. Arch Intern Med 1971;128:453-5.