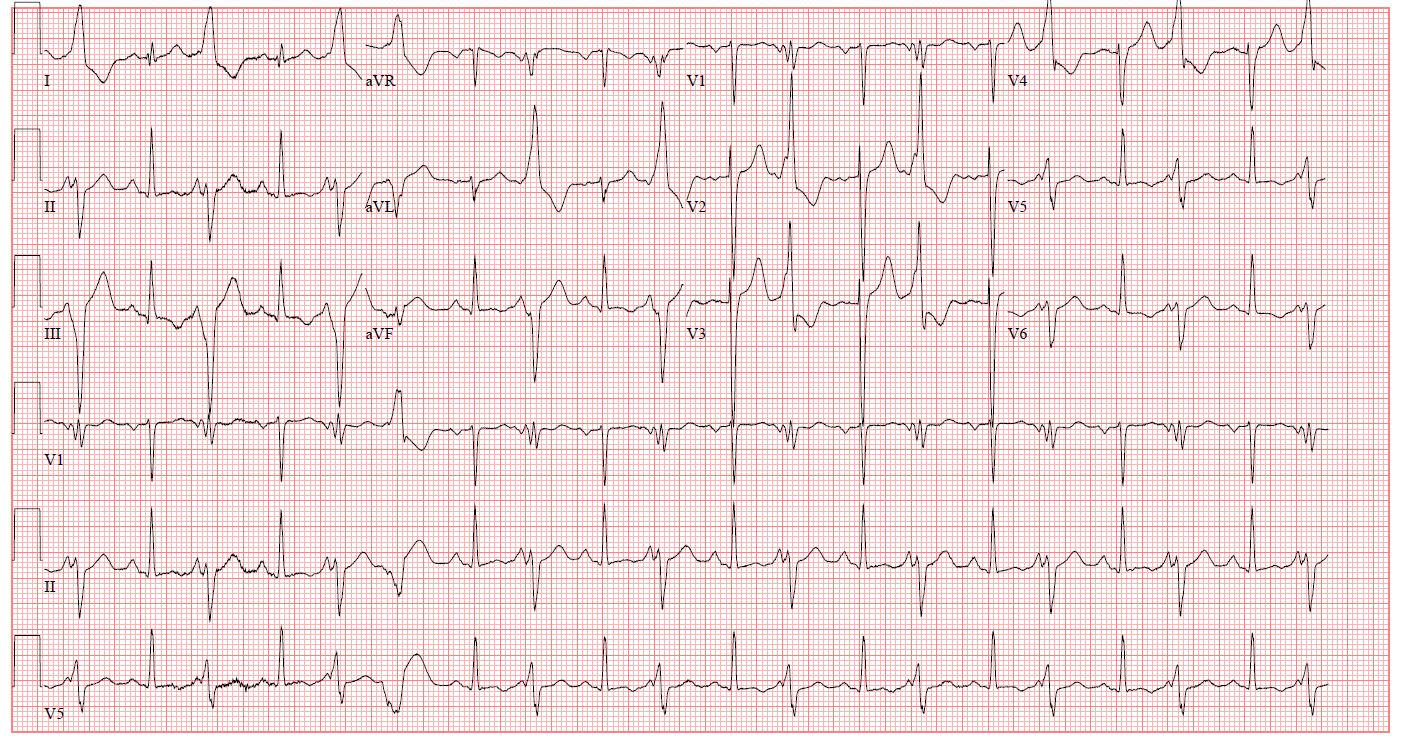
This is a 50-year-old man with a past medical history of chronic systolic heart failure on chronic inotropic therapy who presented with worsening dyspnea over the past two days. A right heart catheterization performed at the time of admission demonstrated a cardiac index of 1.4 and an elevated SVR greater than 2300 Woods units. Medical history is otherwise notable for coronary artery disease, atrial fibrillation, WHO Group II pulmonary hypertension and signet ring adenocarcinoma.
Figure 1
An ECG performed upon admission demonstrates which of the following:
Show Answer
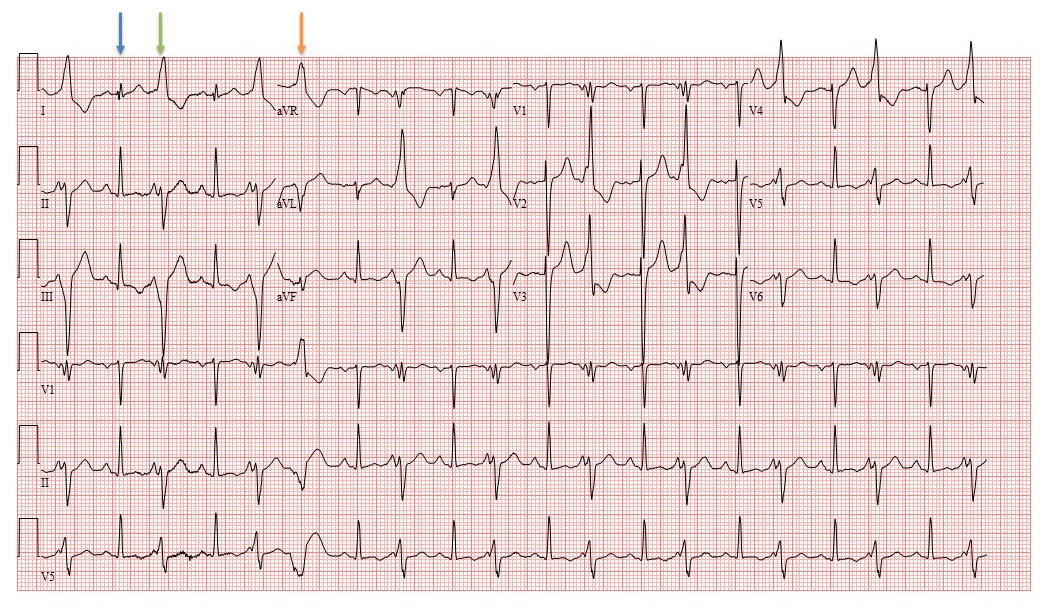
The correct answer is: B. Sinus tachycardia with ventricular ectopy and fusion beats.
The underlying rhythm in this ECG is sinus tachycardia. P waves are present throughout the tracing and there is 1:1 AV conduction with a normal QRS complex (blue arrows) as well as short PR intervals due to fusion beats (green arrows). There is one clearly identifiable premature ventricular beat (orange arrows) with a right bundle morphology with no preceding P wave. There are identical P waves compatible with normal axis indicating a sinus origin before each QRS complex evident in lead II and V5. Therefore, atrial tachycardia is incorrect. This is not electrical alternans because of the variable PR intervals. The consistent morphology of fusion beats suggests a consistent ectopic ventricular focus and rules out polymorphic ventricular tachycardia. This was first reported by William Dressler in 1952 as a way to differentiate supraventricular and ventricular tachycardias.1
Figure 2
References
Dressler W, Roesler H. The occurrence in paroxysmal ventricular tachycardia of ventricular complexes transitional in shape to sinoauricular beats: a diagnostic aid. Am Heart J 1952;44:485-93.