The patient is 75-year-old man with history of end stage renal disease, heart failure with reduced ejection fraction (HFrEF), s/p TAVR for moderately severe aortic stenosis, paroxysmal atrial fibrillation, and s/p left atrial appendage closure device due to GI bleeding, who was admitted to hospital because of acute increase in dyspnea and protracted cough. He was diagnosed with acute on chronic heart failure and troponin at 0.34 [normal < 0.11 ng/ml].
The following ECG was performed (Figure 1):
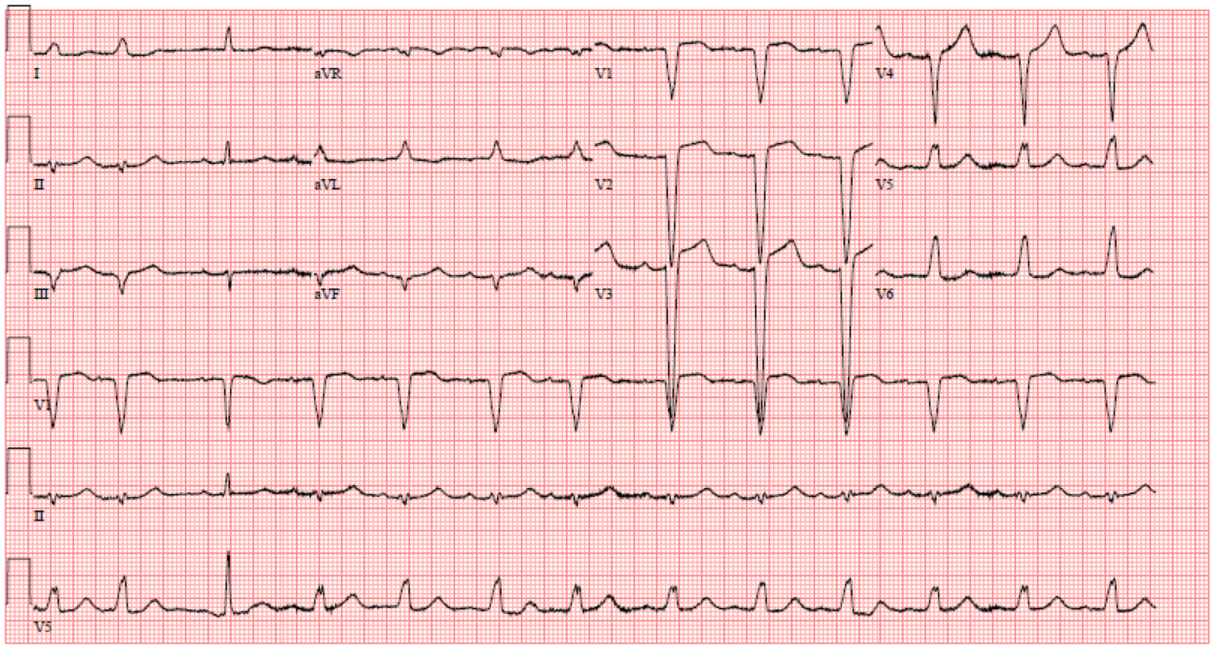
Figure 1
Figure 1
The ECG shows which of the following:
Show Answer
The correct answer is: C. Anterior wall impending injury pattern with left bundle branch block (LBBB).
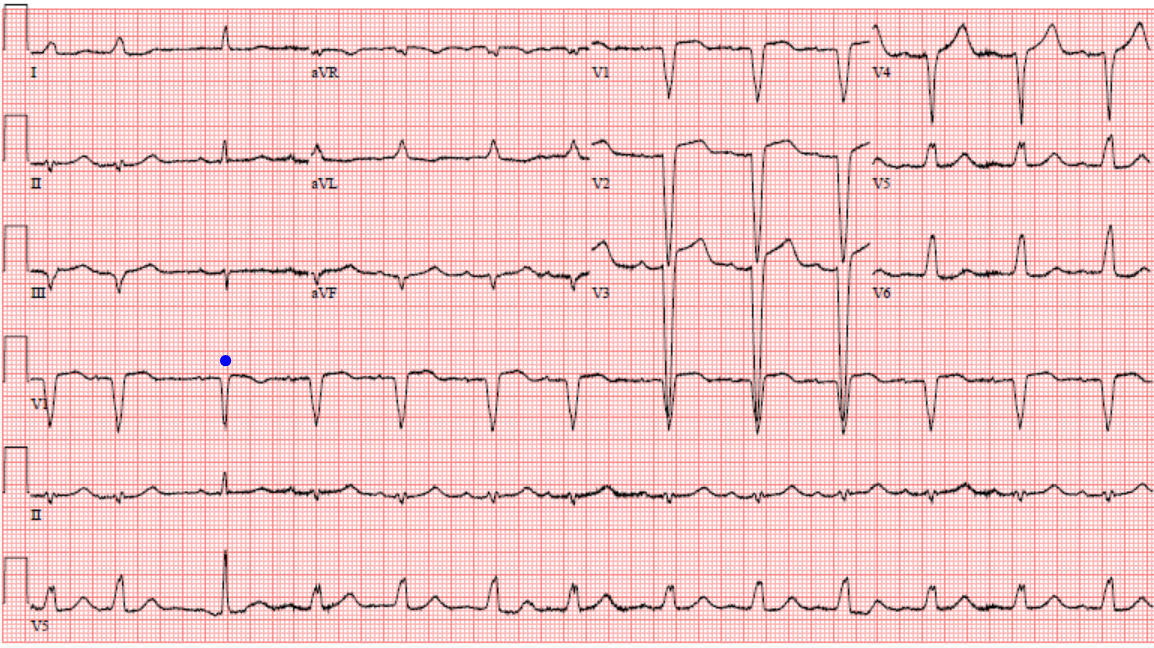
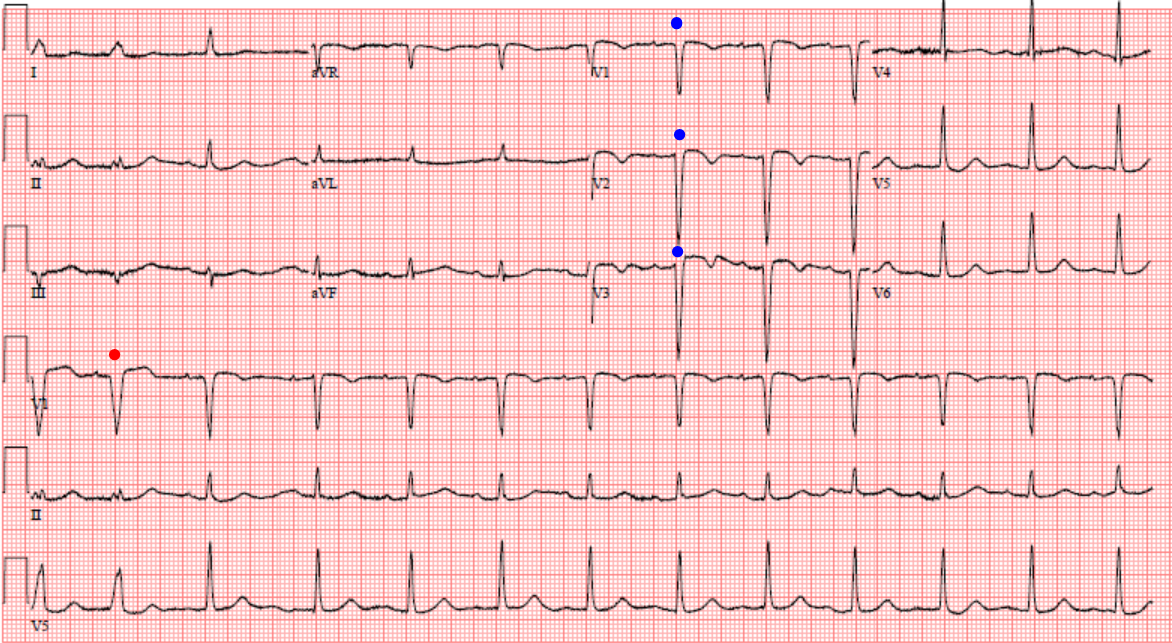
The ECG shows sinus rhythm with narrow QRS as noted on third beat. The reminder of the complexes are wide with LBBB morphology. This is rate related LBBB. Slower heart rate improves the conduction over the LBB, which results in the narrow QRS complex beat. The narrow QRS complex beat shows a horizontal 1mm ST elevation and T wave inversion in V1 which is compatible with an anterior injury (Figure 2; blue dots) and was present in the subsequent ECG (Figure 3), which showed ST elevation and inverted T wave in V1 through V3, which is compatible with antero-septal injury. Left heart catheterization showed a 70% stenosis in the mid left anterior descending (LAD) artery just after the large first diagonal (D1) branch. D1 is larger in size then the LAD and almost serves as a dual LAD; a 60-70% stenosis in the ostial left circumflex (LCx) artery; an 85% stenosis in the right posterior descending artery.
Figure 2
Figure 2
Figure 3
Figure 3
Patient was not a good candidate for coronary artery bypass graft (CABG). Percutaneous coronary intervention (PCI) was not performed due to history of GI bleeding. He was continued on guideline directed medical therapy for HFrEF.
de Zwaan et al.3 reported characteristic ECG pattern in the precordial lead V1-through V3 including horizontal ST elevation and T wave inversion that indicate critical stenosis of the left anterior descending coronary artery [LAD].
Please note the second beat "red dot" in subsequent ECG (Figure 3) has the rate related LBBB morphology.
References
Galeotti L, van Dam PM, Loring Z, Chan D, Strauss DG. Evaluating strict and conventional left bundle branch block criteria using electrocardiographic simulations. Europace 2013;15:1816-1821.
Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2018. [Epub ahead of print]
de Zwaan C, Bar FW, Wellens HJ, et al. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J 1982;103:730-6.