A 90-year-old woman with a past medical history of coronary artery disease with previous coronary artery bypass grafting, heart failure (HF) with preserved ejection fraction, World Health Organization (WHO) grade II pulmonary hypertension, sick sinus syndrome with a dual chamber pacemaker, paroxysmal non-valvular atrial fibrillation, stage 3 chronic kidney disease, hypertension, and hyperlipidemia presents to the hospital with dyspnea and lower extremity edema, consistent with an acute HF exacerbation. She receives intravenous furosemide with improvement in her symptoms. She denies palpitations or syncope.
An electrocardiogram (ECG) is performed on admission (Figure 1).
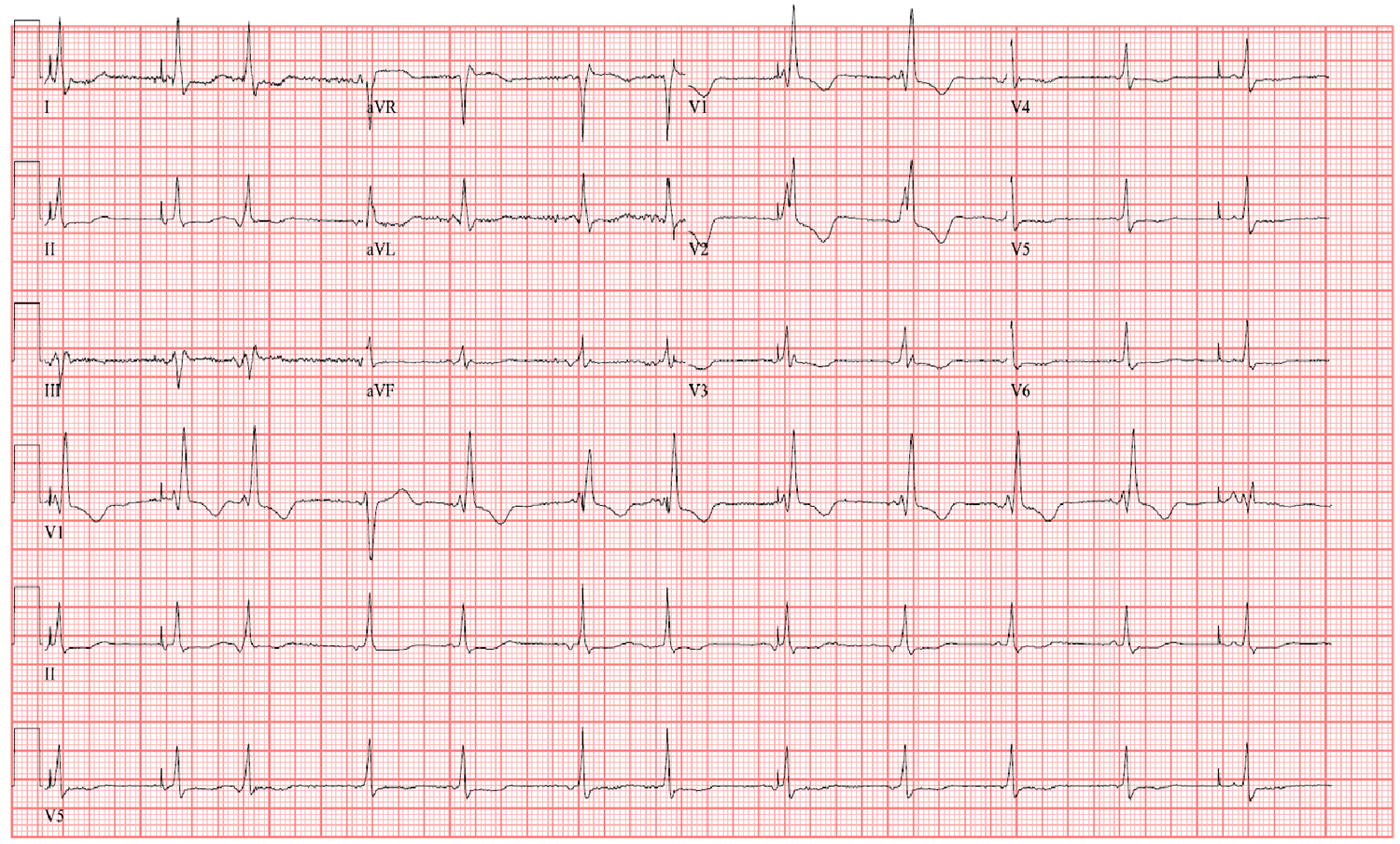
Figure 1
Figure 1
The ECG shows which of the following?
Show Answer
The correct answer is: A. Right atrial pacer undersensing.
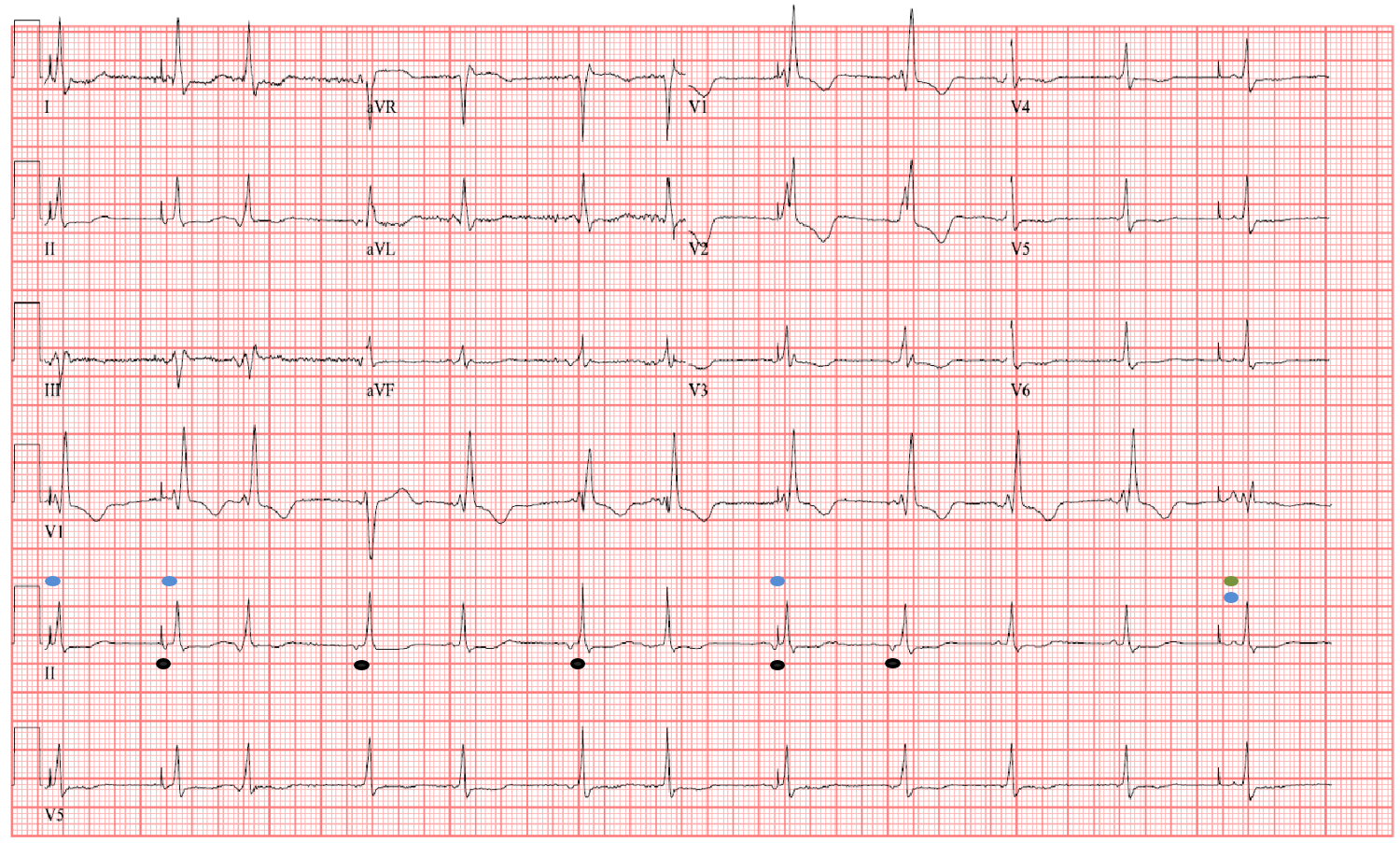
Figure 2
Figure 2
This patient is not consistently capturing or sensing from the right atrial lead of her dual chamber pacemaker. The blue dots in Figure 2 are examples of undersensing by the atrial lead as the pacer spike is after the p-wave. Additionally, there is lack of capture at the green dot in Figure 2 as there is a delay of atrial depolarization following the pacer spike. This patient was found to have a right atrial lead fracture on her pacemaker interrogation.1 She underwent a venogram, and the left subclavian vein was occluded. The patient preferred to proceed with a non-invasive approach to management given her co-morbidities. She was reprogrammed from DDDR to VVIR at 60 bpm.
Answer choice B is an incorrect choice, as right ventricular pacing would cause a left bundle branch block appearance. Answer choice C is an incorrect choice, as the pacer spikes are not artifact, but are the result of the pacemaker lead no consistently capturing. Answer choice D is an incorrect choice because there are P waves prior to each QRS complex, and the irregularities in rhythm are due to PAC's (black dots in Figure 2) as seen by a negative p-wave vector in lead II.
References
Safavi-Naeini, P, Saeed M. Pacemaker Troubleshooting: Common Clinical Scenarios. Tex Heart Inst J 2016;43:415-8.