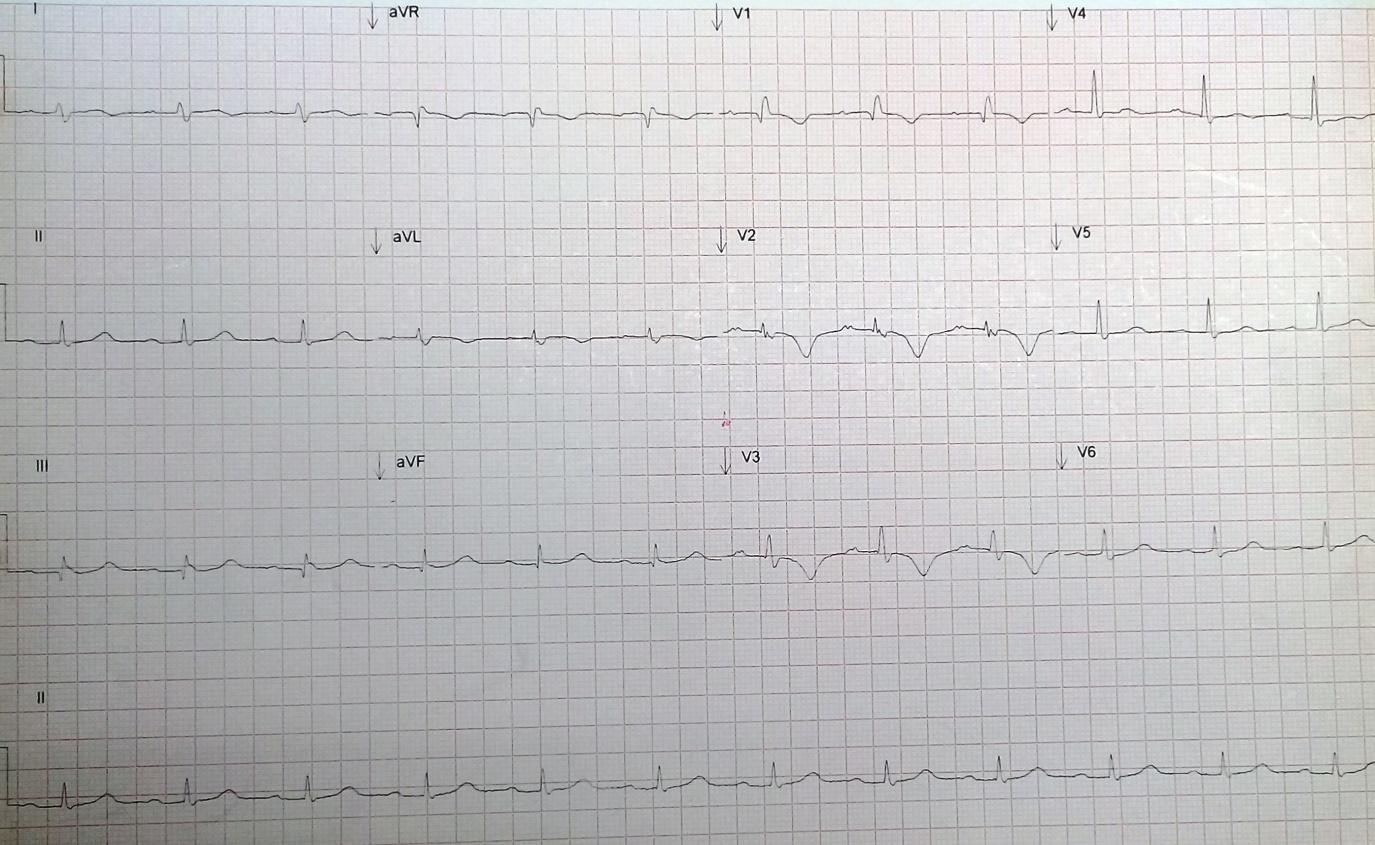
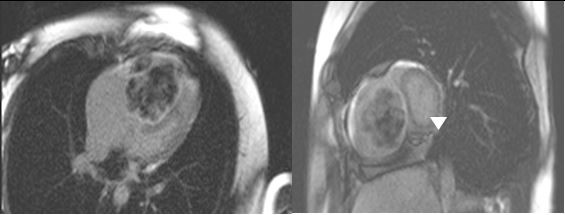
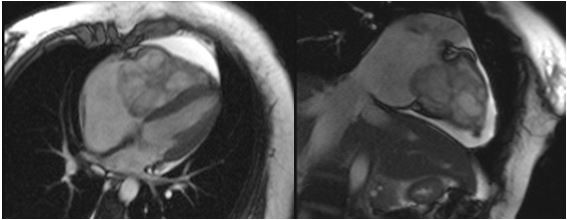
A 20-year-old female patient had a 3-month history of progressive dyspnea. Physical examination showed isolated lentigines of the lower lip, palms of both hands, and left flank. Cardiovascular findings revealed a holosystolic heart murmur at the lower left sterna border. The electrocardiogram was in sinus rhythm with an incomplete right bundle branch block (Figure 1). Transesophageal echocardiogram revealed a right ventricular (RV) hypodense mass of 80 x 57 mm extending through all the RV toward the tricuspid valve with RV outflow tract obstruction and a smaller left ventricular (LV) apical mass of 10 x 10 mm. Severe mitral and tricuspid regurgitation were noted. The initial N-terminal pro b-type natriuretic peptide was 1,465 pg/ml. A contrast computed tomography scan was made, reporting a 22 HU mass in the RV of 50 x 48 x 71 mm that extended to the tricuspid valve; in the apical segment of the LV there was a similar mass of 14 x 15.5 x 12 mm (Figures 2-3).
Figure 1
Figure 1
Figure 2
Figure 2
Figure 3
Figure 3
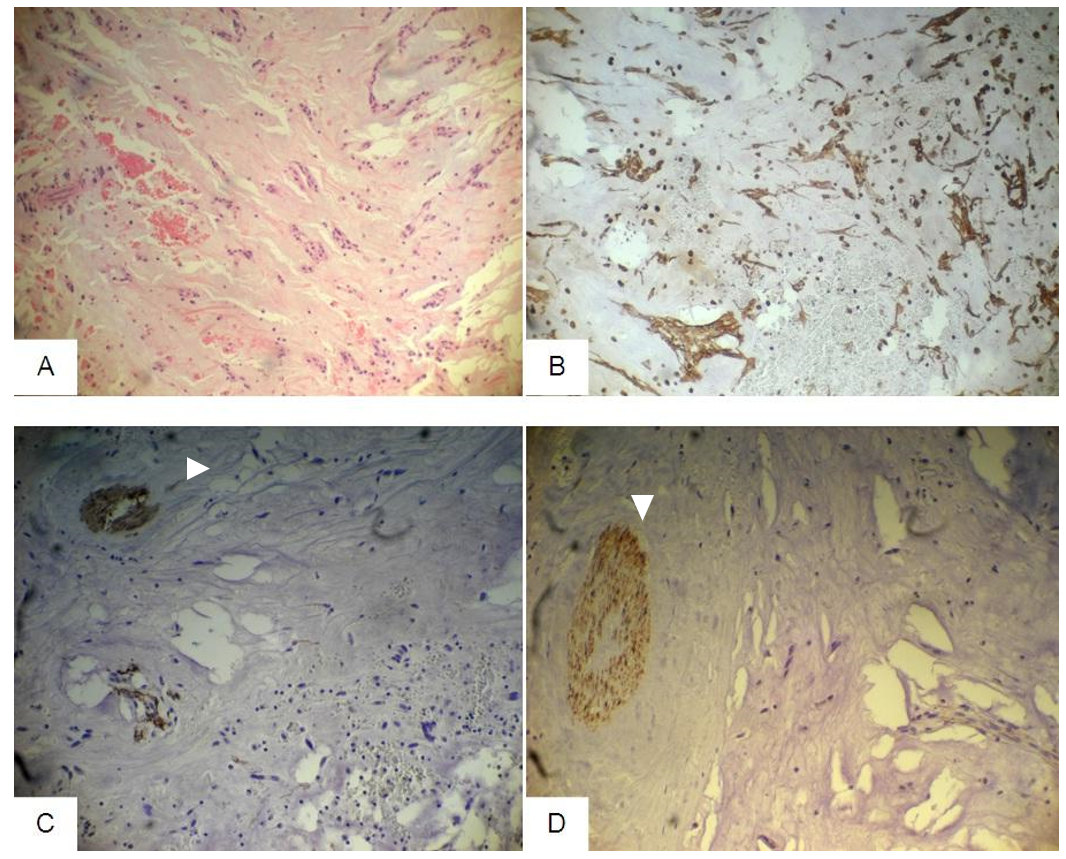
The patient was taken to elective surgery, and the masses were resected and both mitral and tricuspid valves were replaced with bioprostheses (Figure 4). Histopathology confirmed a fragmented myxoma with a hyalinized pedicle without residual endocardial lesions (Figure 5). The complete hormonal panel was normal. Her family was studied. Both of her siblings had ephelides and lentigines; however, there was no evidence of cardiac tumors in any of her relatives. In 2016, the patient had a normal pregnancy with a cesarean section and no complications. Eight months later, a transthoracic echocardiography study showed no residual masses. During her follow-up in 2017, nodular lesions were found in her left breast. A breast ultrasound was revealed multiple nodules, with characteristics of myxomas versus myxoid fibroadenomas.
Figure 4
Figure 4
Macroscopic view of the tumors shows brown reddish color with myxoid and hemorrhagic areas. Left mass corresponds to the myxoma resected from the RV and right mass from the LV.
Macroscopic view of the tumors shows brown reddish color with myxoid and hemorrhagic areas. Left mass corresponds to the myxoma resected from the RV and right mass from the LV.
Figure 5
Figure 5
(A) Hematoxylin-eosin stains 10x microphotography. The tumor is formed of fusiform isolated cells with some cluster of fusiform cells. (B) Vimentin, mesenchymal cells stain in color brown. (C) Anti-Actin specific for smooth muscle staining the wall of the vessels. There is no evidence of malignant cells nor a smooth muscle origin. (D) Desmin stain, negative for malignant cells or striated muscle origin.
(A) Hematoxylin-eosin stains 10x microphotography. The tumor is formed of fusiform isolated cells with some cluster of fusiform cells. (B) Vimentin, mesenchymal cells stain in color brown. (C) Anti-Actin specific for smooth muscle staining the wall of the vessels. There is no evidence of malignant cells nor a smooth muscle origin. (D) Desmin stain, negative for malignant cells or striated muscle origin.
What is this patient's most likely diagnosis?
Show Answer
The correct answer is: B. Carney complex
Primary cardiac tumors are very rare, with an autopsy incidence of 0.001-0.03%, including benign and malignant tumors. Benign tumors are more frequent than malignant tumors, and among them myxomas are the most frequent, with an autopsy incidence of 1.7-14%. Twenty percent of myxomas have been reported in patients with cancer.1 In 1985, Dr. J. Aidan described the association of myxomas, spotty skin pigmentation (lentigines), and endocrine overactivity,2 the first report of what we know today as Carney syndrome. Carney syndrome is a syndrome inherited as an autosomal dominant trait, but sporadic mutations can occur. It is caused by a mutation in the PRKAR1A gene (OMIM 188830) coding for the regulatory subunit type I-alpha of protein kinase A1,2,3 that maps at the 17q24.3 locus.4 Up to 10% of cardiac myxomas occur in the context of Carney syndrome. The diagnosis is made by
the presence of two major criteria confirmed by histology, imaging, or biochemical testing
or one major and one supplemental criterion (Table 1).
The median age at which myxomas are detected is 20 years.2,3,5 There are few data regarding Carney syndrome in women of childbearing age. Staudt et al.6 reported two cases of women with Carney complex. One delivered a healthy baby, with no complications during the procedures. Our patient had a cesarean section with no complication, and during her echocardiographic follow-up, there was no evidence of tumor recurrence. It is important to note that myxomas carry a high risk of embolic events and sudden death due to RV outflow tract obstruction, so it is of major importance that when there is a suspicion of Carney syndrome, further testing is immediately done to prevent fatal complications.
Carney complex is a multidisciplinary disease that should be taken into consideration by a cardiologist, oncologist, and a dermatologist. Some authors recommend at least an annual echocardiogram to patients with this disease, along with regular skin evaluations, complete hormonal testing, and regular physical examination to detect any of the malignant tumors described in Table 1.2,6-9 When a cardiac myxoma is detected, cardiac imaging may be done more frequently, for example biannually. Life expectancy may be high with careful surveillance, with an average lifespan of 50-55 years. The most common causes of death are related to complications of heart myxomas, such as embolic strokes, post-operative cardiomyopathy, and cardiac arrhythmias, as well as metastatic cancer from psammomatous melanotic schwannomas.1,2,9–10
Table 1: Diagnostic Criteria of Carney Complex
The diagnosis is made when the patient exhibits two of the major criteria listed below, or one major criterion and one supplemental criterion.
Major Criteria
Spotty skin pigmentation with a typical distribution (lips, conjunctiva, inner or outer canthi, vaginal and penile mucosa)
Myxoma (cutaneous and mucosal)
Cardiac myxoma
Breast myxomatosis or fat-suppressed magnetic resonance imaging findings suggestive of diagnosis
Primary pigmented nodular adrenocortical disease or paradoxical positive response of urinary glucocorticosteroids to dexamethasone administration during Liddle´s test
Acromegaly due to growth-hormone-producing adenoma
Large-cell calcifying Sertoli cell tumor or characteristic calcification on testicular ultrasonography
Thyroid carcinoma or multiple hypoechoic nodules on thyroid ultrasonography
Psammomatous melanotic schwannoma
Multiple epithelioid blue nevus
Breast ductal adenoma
Osteochondromyxoma of bone
Supplemental Criteria
Affected first-degree relative
Inactivating mutation of the PRKAR1A gene
References
Lenihan DJ, Yusuf SW. "Tumors Affecting the Cardiovascular System" In: Douglas L, Douglas PZ, Peter L, Robert O, Eugene B, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. Philadelphia: Saunders; 2015:1865-6.
Stratakis CA. Carney complex: A familial lentiginosis predisposing to a variety of tumors. Rev Endocr Metab Disord 2016;17:367-71.
Bandettini WP, Karageorgiadis AS, Sinaii N, et al. Growth hormone and risk for cardiac tumors in Carney complex. Endocr Relat Cancer 2016;23:739-46.
Serio A, Favalli V, Giuliani L, et al. Cardio-Oncology: The Carney Complex Type I. J Am Coll Cardiol 2016;68:1921-3.
Di Vito A, Mignogna C, Donato G. The mysterious pathways of cardiac myxomas: a review of histogenesis, pathogenesis and pathology. Histopathology 2015;66:321-32.
Staudt G, Camann W. Successful pregnancy and delivery in a patient with Carney complex: implications for anesthesiologists. A A Case Rep 2015;4:12-3.
Kim H, Cho HY, Lee JN, Park KY. Carney Complex with Multiple Cardiac Myxomas, Pigmented Nodular Adrenocortical Hyperplasia, Epithelioid Blue Nevus, and Multiple Calcified Lesions of the Testis: A Case Report. J Pathol Transl Med 2016;50:312-4.
Feng J. Timely screening for Carney complex and PRKAR1A gene mutations. J Thorac Cardiovasc Surg 2016;152:1440-1.
Maleszewski JJ, Larsen BT, Kip NS, et al. PRKAR1A in the development of cardiac myxoma: a study of 110 cases including isolated and syndromic tumors. Am J Surg Pathol 2014;38:1079-87
Tirosh A, Auerbach A, Bonella B, et al. Failure to Thrive in the Context of Carney Complex. Horm Res Paediatr 2018;89:38-46.