A 62-year-old female presents with NYHA class III dyspnea. She reports no chest discomfort, orthopnea or paroxysmal nocturnal dyspnea. Cardiovascular risk factors include 40 pack-years of tobacco use. Five months prior, she was diagnosed with a stage IIIA T3N1M0G3 esophageal carcinoma and had undergone neoadjuvant chemoradiation therapy with a CROSS-style regimen for a total dose of 41.4Gy in 23 fractions. Concurrent chemotherapy included carboplatin and paclitaxel. On physical examination, she had a blood pressure of 100/60 mmHg and a regular heart rate of 80 beats/min. Jugular venous pressure was 12 cm H2O; however, no Kussmaul sign was detected. Auscultation revealed a normal S1, normal splitting of S2 and an intermittent pericardial rub without a pericardial knock. Laboratory data included a hemoglobin level of 12.4mg/dL, normal WBC count with differential and platelet count. Electrolytes, blood urea nitrogen and creatinine, lipids and liver enzymes were normal. Both erythrocyte sedimentation rate and high-sensitivity C-reactive protein levels were elevated (42 mm/hr and 87 mg/L, respectively). Electrocardiogram showed normal sinus rhythm and inverted T-waves in the inferior and anterolateral leads. Transthoracic echocardiography revealed new pericardial thickening along with a small circumferential pericardial effusion, LVEF of 52%, right ventricular systolic pressure of 42 mmHg and a mildly dilated inferior vena cava (2.3cm, normal range ≤2.1cm) with no inspiratory collapse.
Global averaged left ventricular longitudinal peak systolic strain was -15% (normal more negative than -18%). Doppler assessment with respirometer showed ventricular inter-dependence and diastolic flow reversals in the hepatic veins. Annulus reversus was not present. (Figures 1 and 2)
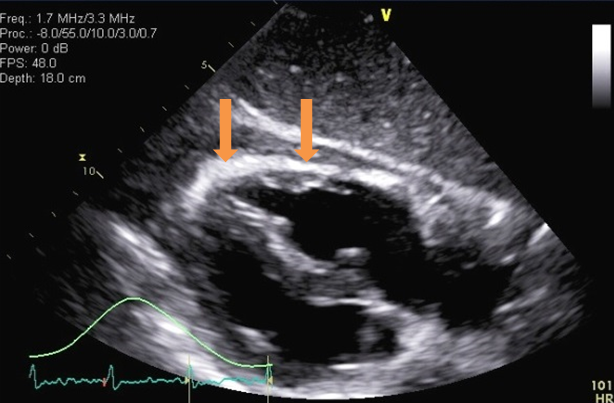
Figure 1
Figure 1: Thickened pericardium (arrows, up to 7mm) as seen on transthoracic echocardiogram, subcostal four chamber view
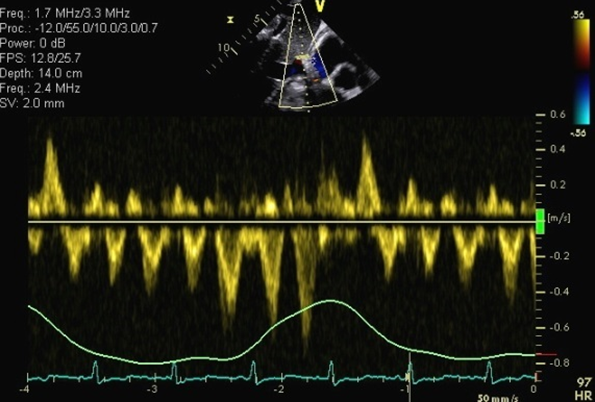
Figure 2
Figure 2: Diastolic flow reversal in hepatic vein Doppler assessment
Which of the following is the most likely diagnosis?
Show Answer
The correct answer is: C. Radiation-induced early constrictive pericarditis.
Cancer patients' survival rates continue to improve in the current era, and radiation therapy (RT) remains prominent in the treatment of many cancers. With this, the number of patients with radiation-induced cardiovascular sequelae is expected to rise.1,2 Acute pericarditis may be seen within a few weeks after RT. Chronic constriction typically occurs decades later, consequent to fibrosis.1-4 Although rare, early pericardial constriction has been reported in a few cases.5
This patient had early onset constrictive pericarditis due to the radiation therapy she received as part of her esophageal cancer treatment. Echo-Doppler findings including diastolic flow reversals in the hepatic veins and ventricular inter-dependence in the setting of thickened pericardium suggest constrictive pericarditis. In this particular case, a thickened pericardium with small circumferential pericardial effusion, temporally associated with recent radiation treatment in the absence of other etiologies of pericarditis, make radiation-induced early constrictive pericarditis the most likely diagnosis.
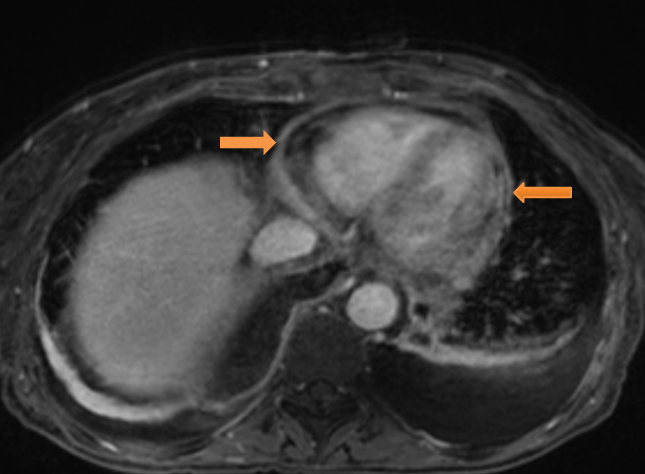
The diagnosis was confirmed on cardiac magnetic resonance (CMR) imaging with gadolinium. There was early gadolinium enhancement consistent with acute/active inflammation, coupled with diffusely thickened pericardium (8mm) and ventricular interdependence on cine images consistent with constrictive pericarditis. LV ejection fraction was normal. (Figures 3 and 4)
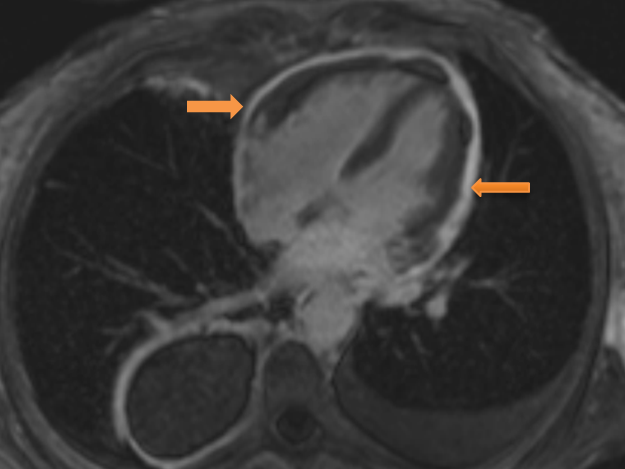
Figure 4: CMR phase sensitive inversion recovery delayed enhancement image in four chamber view showing diffuse circumferential pericardial enhancement (arrows).
While patients with cancer are at risk of venous thromboembolism, there are no supportive clinical and diagnostic imaging findings to suggest the presence of pulmonary embolism in this patient. Ischemic heart disease as a result of radiation induced coronary artery disease usually occurs decades later.1,2 Similarly, while chemotherapy can lead to cardiomyopathy by direct or indirect toxicity to the heart, the decrease in left ventricular systolic function and average global longitudinal strain pattern are only mildly reduced in this patient, making this an unlikely diagnosis. Besides it would not explain the presence of thickened pericardium and elevated inflammatory markers.
The patient was treated with 1.5 mg/kg/d of steroids tapered over 2 months, together with colchicine (0.6 mg/d). After 30 days, the patient's erythrocyte sedimentation rate and high-sensitivity C-reactive protein levels were normal. Upon completion of therapy, her symptoms improved. At 1 and 2 year follow up visits, the patient remains clinically well, with repeat echocardiography showing no evidence of pericardial constriction.
References
Bhattacharya S, Asaithamby A. Inozing radiation and heart risks. Semin Cell Dev Biol 2016;58:14-25.
Groarke JD, Nguyen PL, Nohria A, Ferrari R, Cheng S, Moslehi J. Cardiovascular complications of radiation therapy for thoracic malignancies: the role for non-invasive imaging for detection of cardiovascular disease. Eur Heart J 2014;35:612-23.
Stewart FA, Seemann I, Hoving S, Russell NS. Understanding radiation-induced cardiovascular damage and strategies for intervention. Clin Oncol (R Coll Radiol) 2013;25:617-24.
Gaya AM, Ashford RF. Cardiac complications of radiation therapy. Clin Oncol (R Coll Radiol) 2005;17:153-9.
Yeneneh BT, Allen S, Panse P, Mookadam F, Rule W. Constrictive pericarditis 5 months after radiation therapy in a 62-year-old woman with esophageal cancer. Tex Heart Inst J 2017;44:411-5.