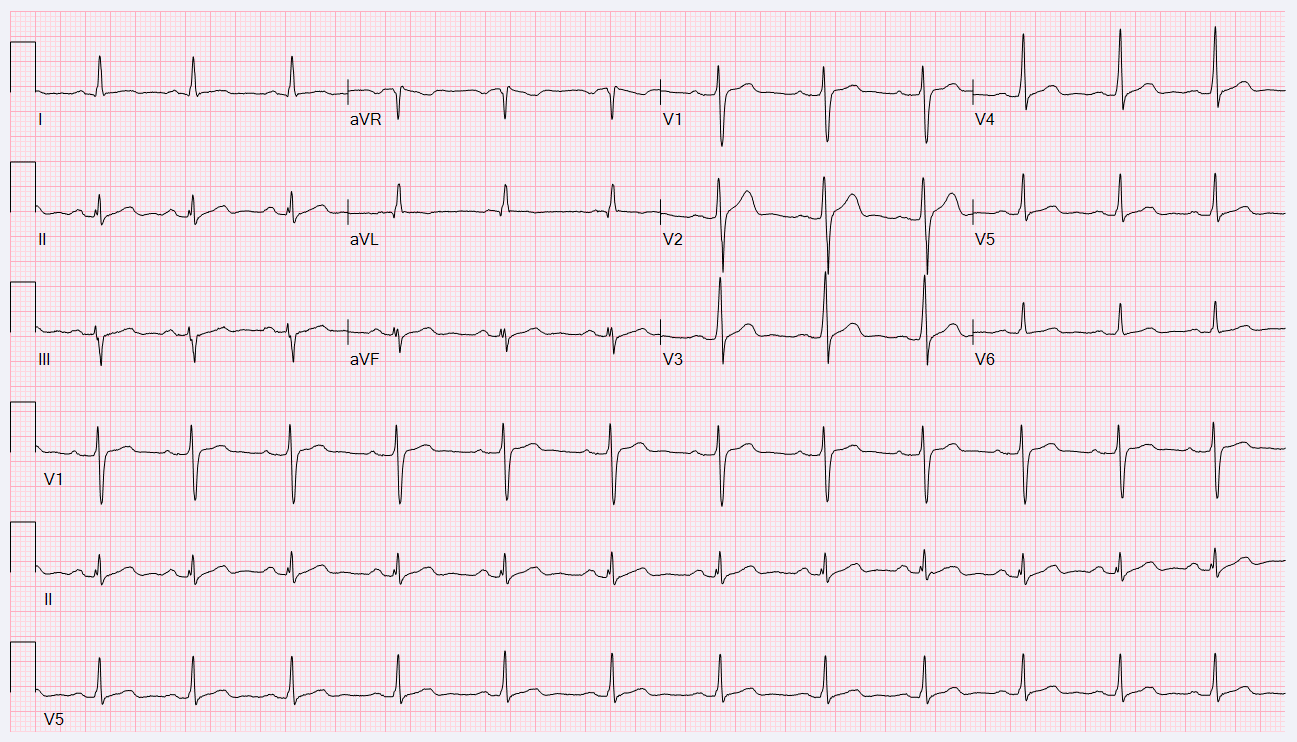
A 21-year-old white male presented to the emergency department after ingesting excessive alcohol in combination with bupropion, which he takes for depression. He is a recreational athlete. He has no other medical problems and is unable to provide a family history. He denied any history of palpitations or syncope. An ECG was obtained on admission:
Another ECG was obtained 12 hours later:
Which of the following is the correct diagnosis?
Show Answer
The correct answer is: A. Spontaneous Type I Brugada ECG pattern.
This patient has a spontaneous, albeit transient, Type I Brugada ECG pattern. Brugada syndrome (BrS) is characterized by an rSr' pattern in the right precordial leads on ECG.1,2 The Type I Brugada ECG pattern (BrEP) has a coved ST segment elevation ≥2 mm followed by a symmetric negative T wave and, alone, is considered diagnostic.2,3 The classic Type 2 BrEP has a saddleback appearance with an r' in the right precordial leads, convex ST-elevation ≥0.5 mm with a positive T wave in lead V2, and variable morphology in lead V1.2,3 The BrEP is often concealed and can be unmasked by medications and toxins such as sodium channel blockers and alcohol as well as febrile states, hyperkalemia, hypokalemia, and hypercalcemia.4 Of note, alcohol and bupropion are both contraindicated in patients with Brugada syndrome as they can unmask the ECG findings.5 The clinical presentation of BrS includes ventricular tachyarrhythmias, sudden cardiac arrest, syncope, chest discomfort, and nocturnal agonal respirations.1 Many patients, however, are asymptomatic and are diagnosed after incidental ECG findings. According to the 2013 HRS/EHRA/APHRS consensus statement, Brugada syndrome is diagnosed when a Type I ST-segment elevation is observed spontaneously or after IV administration of a sodium channel blocking agent, such as procainamide, in V1 and/or V2 (placed in a standard or a superior position up to the 2nd intercostal space).1
After being discharged from the ED, the patient saw an electrophysiologist for further evaluation. After underlying structural heart disease was ruled out with echocardiography, a drug challenge with procainamide 10 mg/kg over 10 minutes was performed with continuous ECG monitoring.
Before procainamide:
After procainamide:
Implantable cardioverter defibrillators (ICD) are the only proven therapy for the prevention of sudden cardiac death in patients with BrS. ICDs, however, are not indicated in patients with asymptomatic BrS with a drug-induced type 1 ECG.1 Therefore, the best recommendation for this patient is avoidance of sodium channel blocking medications and aggressive fever treatment. Of note, genetic testing was performed and returned positive for a pathologic, truncating SCN5A mutation associated with Brugada syndrome.
References
Priori SG, Wilde AA, Horie M, et al. HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes: document endorsed by HRS, HERA, and APHRS in May 2013 and by ACCF, AHA, PACES, and AEPC in June 2013. Heart Rhythm 2013;10:1932-63.
Chung EH. Brugada ECG patterns in athletes. J Electrocardiol 2015;48:539-43.
Baranchuk A, Enriquez A, Garcia-Niebla J, Bayes-Genis A, Villuendas R, Bayes de Luna A. Differential diagnosis of rsr' pattern in leads V1-V2. Comprehensive review and proposed algorithm. Ann Noninvasive Electrocardiol 2015;20:7-17.
Antzelevitch C, Brugada P, Borggrefe M, et al. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation 2005;111:659-70.